
Loading, please wait.
By using this website, you are agreeing to our terms of use.
Loading, please wait.
Atlas Table of Contents
Osteology.
The Skeleton of the Trunk.
Fig. A1
Fig. A2
Fig. A3
Fig. A4
Fig. A5
Fig. A6
Fig. A7
Fig. A8
Fig. A9
Fig. A10
Fig. A11
Fig. A12
Fig. A13
Fig. A14
Fig. A15
Fig. A16
Fig. A17
Fig. A18
Fig. A19
Fig. A20
Fig. A21
Fig. A22
Fig. A23
Fig. A24
Fig. A25
Fig. A26
Fig. A27
Fig. A28
Fig. A29
Fig. A30
Fig. A31
Fig. A32
Fig. A33
Fig. A34
Fig. A35
Fig. A36
Fig. A37
Fig. A38
Fig. A39
Fig. A40
Fig. A41
The Skull and the Skull Bones.
Fig. A42
Fig. A43
Fig. A44
Fig. A45
Fig. A46
Fig. A47
Fig. A48
Fig. A49
Fig. A50
Fig. A51
Fig. A52
Fig. A53
Fig. A54
Fig. A55
Fig. A56
Fig. A57
Fig. A58
Fig. A59
Fig. A60
Fig. A61
Fig. A62
Fig. A63
Fig. A64
Fig. A65
Fig. A66
Fig. A67
Fig. A68
Fig. A69
Fig. A70
Fig. A71
Fig. A72
Fig. A73
Fig. A74
Fig. A75
Fig. A76
Fig. A77
Fig. A78
Fig. A79
Fig. A80
Fig. A81
Fig. A82
Fig. A83
Fig. A84
Fig. A85
Fig. A86
Fig. A87
Fig. A88
Fig. A89
Fig. A90
Fig. A91
Fig. A92
Fig. A93
Fig. A94
Fig. A95
Fig. A96
Fig. A97
Fig. A98
Fig. A99
Fig. A100
Fig. A101
Fig. A102
Fig. A103
Fig. A104
Fig. A105
Fig. A106
Fig. A107
Fig. A108
Fig. A109
Fig. A110
Fig. A111
Fig. A112
Fig. A113
Fig. A114
Fig. A115
The Appendicular Skeleton.
Fig. A116
Fig. A117
Fig. A118
Fig. A119
Fig. A120
Fig. A121
Fig. A122
Fig. A123
Fig. A124
Fig. A125
Fig. A126
Fig. A127
Fig. A128
Fig. A129
Fig. A130
Fig. A131
Fig. A132
Fig. A133
Fig. A134
Fig. A135
Fig. A136
Fig. A137
Fig. A138
Fig. A139
Fig. A140
Fig. A141
Fig. A142
Fig. A143
Fig. A144
Fig. A145
Fig. A146
Fig. A147
Fig. A148
Fig. A149
Fig. A150
Fig. A151
Fig. A152
Fig. A153
Fig. A154
Fig. A155
Fig. A156
Fig. A157
Fig. A158
Fig. A159
Fig. A160
Fig. A161
Fig. A162
Fig. A163
Fig. A164
Fig. A165
Fig. A166
Fig. A167
Fig. A168
Fig. A169
Fig. A170
Fig. A171
Fig. A172
Fig. A173
Fig. A174
Fig. A175
Bone Structure.
Fig. A176
Fig. A177
Fig. A178
Fig. A179
Fig. A180
Fig. A181
Röntgen Pictures of the Human Skeleton.
Fig. A182
Fig. A183
Fig. A184
Fig. A185
Fig. A186
Fig. A187
Fig. A188
Fig. A189
Fig. A190
Syndesmology.
Joints and Ligaments of the Trunk and Head.
Fig. A191
Fig. A192
Fig. A193
Fig. A194
Fig. A195
Fig. A196
Fig. A197
Fig. A198
Fig. A199
Fig. A200
Fig. A201
Fig. A202
Fig. A203
Fig. A204
Fig. A205
Fig. A206
Fig. A207
Fig. A208
Fig. A209
Fig. A210
Fig. A211
Joints and Ligaments of the Upper Extremity.
Fig. A212
Fig. A213
Fig. A214
Fig. A215
Fig. A216
Fig. A217
Fig. A218
Fig. A219
Fig. A220
Fig. A221
Fig. A222
Fig. A223
Fig. A224
Fig. A225
Joints and Ligaments of the Lower Extremity.
Fig. A226
Fig. A227
Fig. A228
Fig. A229
Fig. A230
Fig. A231
Fig. A232
Fig. A233
Fig. A234
Fig. A235
Fig. A236
Fig. A237
Fig. A238
Fig. A239
Fig. A240
Fig. A241
Fig. A242
Fig. A243
Fig. A244
Fig. A245
Fig. A246
Fig. A247
Fig. A248
Fig. A249
Fig. A250
Fig. A251
Myology.
Muscles of the Back.
Fig. A252
Fig. A253
Fig. A254
Fig. A255
Fig. A256
Fig. A257
Fig. A258
Fig. A259
Fig. A260
Muscles of the Thorax and Abdomen, including the Diaphragm and Iliopsoas.
Fig. A261
Fig. A262
Fig. A263
Fig. A264
Fig. A265
Fig. A266
Fig. A267
Fig. A268
Fig. A269
Fig. A270
Pl. A1, Fig. 1
Pl. A1, Fig. 2
Muscles of the Neck.
Fig. A271
Fig. A272
Fig. A273
Fig. A274
Fig. A275
Fig. A276
Muscles of the Head.
Fig. A277
Fig. A278
Fig. A279
Fig. A280
Fig. A281
Fig. A282
Muscles and Fasciae of the Upper Extremity.
Fig. A283
Fig. A284
Fig. A285
Fig. A286
Fig. A287
Fig. A288
Fig. A289
Fig. A290
Fig. A291
Fig. A292
Fig. A293
Fig. A294
Fig. A295
Fig. A296
Fig. A297
Fig. A298
Fig. A299
Fig. A300
Fig. A301
Fig. A302
Fig. A303
Fig. A304
Fig. A305
Fig. A306
Fig. A307
Fig. A308
Pl. A2, Fig. 1
Pl. A2, Fig. 2
Muscles and Fasciae of the Lower Extremity.
Fig. A309
Fig. A310
Fig. A311
Fig. A312
Fig. A313
Fig. A314
Fig. A315
Fig. A316
Fig. A317
Fig. A318
Fig. A319
Fig. A320
Fig. A321
Fig. A322
Fig. A323
Fig. A324
Fig. A325
Fig. A326
Fig. A327
Fig. A328
Fig. A329
Fig. A330
Fig. A331
Fig. A332
Fig. A333
Fig. A334
Fig. A335
Fig. A336
Fig. A337
Pl. A3, Fig. 1
Pl. A3, Fig. 2
Pl. A4, Fig. 1
Pl. A4, Fig. 2
Regions of the Body.
Fig. A338
Fig. A339
Fig. A340
Fig. A341
Fig. A342
Splanchnology.
Digestive Organs.
Fig. B1
Fig. B2
Fig. B3
Fig. B4
Fig. B5
Fig. B6
Fig. B7
Fig. B8
Fig. B9
Fig. B10
Fig. B11
Fig. B12
Fig. B13
Fig. B14
Fig. B15
Fig. B16
Fig. B17
Fig. B18
Fig. B19
Fig. B20
Fig. B21
Fig. B22
Fig. B23
Fig. B24
Fig. B25
Fig. B26
Fig. B27
Fig. B28
Fig. B29
Fig. B30
Fig. B31
Fig. B32
Fig. B33
Fig. B34
Fig. B35
Fig. B36
Fig. B37
Fig. B38
Fig. B39
Fig. B40
Fig. B41
Fig. B42
Fig. B43
Fig. B44
Fig. B45
Fig. B46
Fig. B47
Fig. B48
Fig. B49
Fig. B50
Fig. B51
Fig. B52
Fig. B53
Fig. B54
Fig. B55
Fig. B56
Fig. B57
Fig. B58
Fig. B59
Fig. B60
Fig. B61
Fig. B62
Fig. B63
Fig. B64
Fig. B65
Fig. B66
Fig. B67
Fig. B68
Fig. B69
Fig. B70
Fig. B71
Fig. B72
Fig. B73
Fig. B74
Fig. B75
Fig. B76
Fig. B77
Fig. B78
Fig. B79
Fig. B80
Fig. B81
Fig. B82
Fig. B83
Fig. B84
Fig. B85
Fig. B86
Fig. B87
Fig. B88
Fig. B89
Fig. B90
Peritoneum and situs viscerum.
Fig. B91
Fig. B92
Fig. B93
Fig. B94
Fig. B95
Fig. B96
Fig. B97
Fig. B98
Fig. B99
Fig. B100
Fig. B101
Fig. B102
Fig. B103
Fig. B104
Fig. B105
Fig. B106
Fig. B107
Fig. B108
Fig. B109
Fig. B110
Fig. B111
Respiratory Organs (including pleura).
Fig. B112
Fig. B113
Fig. B114
Fig. B115
Fig. B116
Fig. B117
Fig. B118
Fig. B119
Fig. B120
Fig. B121
Fig. B122
Fig. B123
Fig. B124
Fig. B125
Fig. B126
Fig. B127
Fig. B128
Fig. B129
Fig. B130
Fig. B131
Fig. B132
Fig. B133
Fig. B134
Fig. B135
Fig. B136
Fig. B137
Fig. B138
Fig. B139
Fig. B140
Fig. B141
Fig. B142
Fig. B143
Fig. B144
Fig. B145
Fig. B146
Fig. B147
Fig. B148
Fig. B149
Fig. B150
Fig. B151
Fig. B152
Fig. B153
Fig. B154
Fig. B155
Fig. B156
Fig. B157
Fig. B158
Fig. B159
Fig. B160
Fig. B161
Fig. B162
Fig. B163
Fig. B164
Fig. B165
Fig. B166
Urogenital Organs, apparatus urogenitalis.
Excretory Organs (including Suprarenal glands).
Fig. B167
Fig. B168
Fig. B169
Fig. B170
Fig. B171
Fig. B172
Fig. B173
Fig. B174
Fig. B175
Fig. B176
Fig. B177
Fig. B178
Fig. B179
Fig. B180
Fig. B181
Fig. B182
Fig. B183
Fig. B184
The Male Genitalia.
Fig. B185
Fig. B186
Fig. B187
Fig. B188
Fig. B189
Fig. B190
Fig. B191
Fig. B192
Fig. B193
Fig. B194
Fig. B195
Fig. B196
Fig. B197
Fig. B198
Fig. B199
Fig. B200
Fig. B201
Fig. B202
Fig. B203
The Female Genitalia.
Fig. B204
Fig. B205
Fig. B206
Fig. B207
Fig. B208
Fig. B209
Fig. B210
Fig. B211
Fig. B212
Fig. B213
Fig. B214
Fig. B215
Fig. B216
Fig. B217
Fig. B218
Fig. B219
Perineum.
Fig. B220
Fig. B221
Fig. B222
Fig. B223
Fig. B224
Angiology and Neurology
The Circulation of the Blood.
Fig. B225
Fig. C1
The Heart.
Fig. B226
Fig. B227
Fig. B228
Fig. B229
Fig. B230
Fig. B231
Fig. B232
Fig. B233
Fig. B234
Fig. B235
Fig. B236
Fig. B237
Fig. B238
Fig. B239
Fig. B240
Fig. B241a
Fig. B241b
Fig. B242
Fig. B243
Fig. B244
The Fetal Circulation.
Fig. C2
Fig. C3
Vessels of the Heart.
Fig. C4
Fig. C5
Nerves and Vessels of the Neck, Axilla, Back and Thoracic Wall.
Fig. C6
Fig. C7
Fig. C8
Fig. C9
Fig. C10
Fig. C11
Fig. C12
Fig. C13
Fig. C14
Fig. C15
Fig. C16
Fig. C17
Fig. C18
Fig. C19
Fig. C20
Fig. C21
Fig. C22
Fig. C23
Fig. C24
Fig. C25
Fig. C26
Fig. C27
Nerves and Vessels of the Upper Extremity.
Fig. C28
Fig. C29
Fig. C30
Fig. C31
Fig. C32
Fig. C33
Fig. C34
Fig. C35
Fig. C36
Fig. C37
Fig. C38
Fig. C39
Fig. C40
Fig. C41
Fig. C42
Fig. C43
Fig. C44
Fig. C45
Fig. C46
Fig. C47
Fig. C48
Fig. C49
Fig. C50
Nerves and Vessels of the Head and the Viscera of the Head and Neck.
Fig. C51
Fig. C52
Fig. C53
Fig. C54
Fig. C55
Fig. C56
Fig. C57
Fig. C58
Fig. C59
Fig. C60
Fig. C61
Fig. C62
Fig. C63
Fig. C64
Fig. C65
Fig. C66
Fig. C67
Fig. C68
Fig. C69
Fig. C70
Fig. C71
Fig. C72
Fig. C73
Fig. C74
Fig. C75
Vessels of the Abdominal Viscera.
Fig. C76
Fig. C77
Fig. C78
Fig. C79
Vessels and Nerves of the false and true Pelvis and of the Perineum.
Fig. C80
Fig. C81
Fig. C82
Fig. C83
Fig. C84
Fig. C85
Fig. C86
Fig. C87
Fig. C88
Fig. C89
Fig. C90
Nerves and Vessels of the Lower Extremity.
Fig. C91
Fig. C92
Fig. C93
Fig. C94
Fig. C95
Fig. C96
Fig. C97
Fig. C98
Fig. C99
Fig. C100
Fig. C101
Fig. C102
Fig. C103
Fig. C104
Fig. C105
Fig. C106
Fig. C107
Fig. C108
Fig. C109
Fig. C110
Fig. C111
Fig. C112
Fig. C113
The Sympathetic Nervous System.
Fig. C114
Fig. C115
Fig. C116
Fig. C117
Fig. C118
The Spinal Cord.
Fig. C119
Fig. C120
Fig. C121
Fig. C122
Fig. C123
Fig. C124
Fig. C125
Fig. C126
Fig. C127
Fig. C128
Fig. C129
Fig. C130
Fig. C131
Fig. C132
Fig. C133
Fig. C134
Meninges and Vessels of the Brain.
Fig. C135
Fig. C136
Fig. C137
Fig. C138
Fig. C139
Fig. C140
Fig. C141
Fig. C142
Fig. C143
Fig. C144
Fig. C145
Fig. C146
Fig. C147
The Brain.
Fig. C148
Fig. C149
Fig. C150
Fig. C151
Fig. C152
Fig. C153
Fig. C154
Fig. C155
Fig. C156
Fig. C157
Fig. C158
Fig. C159
Fig. C160
Fig. C161
Fig. C162
Fig. C163
Fig. C164
Fig. C165
Fig. C166
Fig. C167
Fig. C168
Fig. C169
Fig. C170
Fig. C171
Fig. C172
Fig. C173
Fig. C174
Fig. C175
Fig. C176
Fig. C177
Fig. C178
Fig. C179
Fig. C180
Fig. C181
Fig. C182
Fig. C183
Fig. C184
Fig. C185
Fig. C186
Fig. C187
Fig. C188
Fig. C189
Fig. C190
Fig. C191
Fig. C192
Fig. C193
Fig. C194
Fig. C195
Fig. C196
Fig. C197
Fig. C198
Fig. C199
Fig. C200
Fig. C201
Fig. C202
Fig. C203
Fig. C204
Fig. C205
Fig. C206
Fig. C207
Fig. C208
Fig. C209
Fig. C210
Fig. C211
Fig. C212
Fig. C213
Fig. C214
Fig. C215
Fig. C216
Fig. C217
Fig. C218
Fig. C219
Fig. C220
Fig. C221
Fig. C222
Fig. C223
Fig. C224
Fig. C225
Fig. C226
Fig. C227
Fig. C228
Fig. C229
Fig. C230
Fig. C231
Fig. C232
Fig. C233
Fig. C234
Fig. C235
Sense Organs.
The Eye.
Fig. C236
Fig. C237
Fig. C238
Fig. C239
Fig. C240
Fig. C241
Fig. C242
Fig. C243
Fig. C244
Fig. C245
Fig. C246
Fig. C247
Fig. C248
Fig. C249
Fig. C250
Fig. C251
Fig. C252
Fig. C253
Fig. C254
Fig. C255
Fig. C256
Fig. C257
Fig. C258
Fig. C259
Fig. C260
Fig. C261
Fig. C262
Fig. C263
Fig. C264
Fig. C265
Fig. C266
Fig. C267
Fig. C268
Fig. C269
Fig. C270
Fig. C271
Fig. C272
Fig. C273
Fig. C274
Fig. C275
Fig. C276
Fig. C277
Fig. C278
Fig. C279
Fig. C280
Fig. C281
Fig. C282
Fig. C283
Fig. C284
The Ear.
Fig. C285
Fig. C286
Fig. C287
Fig. C288
Fig. C289
Fig. C290
Fig. C291
Fig. C292
Fig. C293
Fig. C294
Fig. C295
Fig. C296
Fig. C297
Fig. C298
Fig. C299
Fig. C300
Fig. C301
Fig. C302
Fig. C303
Fig. C304
Fig. C305
Fig. C306
Fig. C307
Fig. C308
Fig. C309
Fig. C310
Fig. C311
Fig. C312
Fig. C313
Fig. C314
Fig. C315
Fig. C316
Fig. C317
Fig. C318
Fig. C319
Fig. C320
Fig. C321
Fig. C322
Fig. C323
Fig. C324
Fig. C325
Fig. C326
Fig. C327
Fig. C328
Fig. C329
Fig. C330
Fig. C331
Fig. C332
Fig. C333
Fig. C334
Fig. C335
Fig. C336
Fig. C337
Fig. C338
Fig. C339
The Integument.
Fig. C340
Fig. C341
Fig. C342
Fig. C343
Fig. C344
Fig. C345
Fig. C346
Fig. C347
Fig. C348
Fig. C349
Fig. C350
Fig. C351
Fig. C352
Fig. C353
Lymphatic System.
Fig. C354
Fig. C355
Fig. C356
Fig. C357
Fig. C358
Fig. C359
Fig. C360
Fig. C361
Textbook Table of Contents
I have endeavored in this work to produce an Atlas that will serve the practical needs of students of medicine and practicing physicians. It is not intended to be an Atlas for the use of experts in Anatomy. Consequently in the make-up of the book a limitation to what was absolutely necessary seemed to me a prime consideration.
In its outward form this first volume of the work is treated throughout as an Atlas, is arranged primarily for use by classes in dissection and follows closely the usual methods employed in such classes. Any difficulty that might arise for the beginner by an unusual method of presentation of the figures has, therefore, been carefully avoided.
The illustrations are so arranged that there is to be found on the opposite page, in addition to the explanation of the figures, a brief descriptive text. This enables the student using the book during his dissection to review rapidly the chief points in his preparation. In the Myology the explanatory text takes the form of tables which give at a glance the origin, insertion, nerve supply and action of the muscles. As regards the methods of reproduction of the figures, polychromatic lithography is used for the first time - so far as I am aware - in anatomical illustrations. Of the 34 colored plates 30 are reproduced by this process, the remaining 4 by the method of three (four)- color printing, again used for the first time in this connection. Nearly all the figures in the Myology are reproduced in this manner. For the other illustrations the so-called autotype process is used, and its suitability for the purpose may be seen from the Atlas itself. In addition key-figures, diagrams, etc. have been reproduced by line etching.
For greater convenience special colors have been extensively used in the illustrations reproduced by the autotype process, a chamois tint for the bones in illustrations of the articulations and many of the muscle figures, different colors for the individual skull bones in representations of the entire skull and in topographic figures of the skull bones. For the names of parts the Basel Nomenclature has been used.
The publishers have spared no pains in producing a book that certainly surpasses in excellence of reproduction all previous works, while at the same time it does not materially fall behind the most of them in the number of illustrations.
Würzburg, October 1903.
The Author.
The second edition of the first volume shows very important changes. In the first place the former lithographed plates of the Myology have been entirely omitted and replaced by polychromatic autotypes, as had already been done in the second and third volumes of the first edition. This was done partly for uniformity in reproduction, partly because the illustrations of the first volume were not pleasing to many readers on account of the colors being too bright and glaring on the white paper. I have especially decided to provide new illustrations of the muscles, since those of the first edition frequently did not give a sufficiently natural impression owing to the position of the cadaver. Instead of using photographs of the cadaver, those of an athletic man of small stature were taken as a foundation. These photographs were prepared by the illustrator Mr. K. Hajek and within outlines prepared from them the muscles were drawn from dissections. In this way one obtains correct and expressive figures which, furthermore, are more in keeping with the format of the book. The use of yellow, red and blue colors is naturally merely conventional, although they approximate the natural tints. At the same time the number of the illustrations for the Myology was considerably increased and, furthermore, for the trunk, and especially the thorax and abdomen three-quarter views were employed instead of complete profiles. Mr. K. Hajek has drawn the illustrations in a thoroughly satisfactory manner.
The portions of the book dealing with the Osteology and Syndesmology have also been expanded in various places.
Würzburg, July 1913.
The Author.
Unlike the earlier editions the seventh and eighth have undergone some not unimportant changes. Some Röntgen figures from Grashey's Atlas have been included, new figures of the muscles of the neck and face replace the older ones and a number of the osteological figures have been renewed. In correspondence with these changes the text has been somewhat enlarged.
Bonn, November 1929 and February 1932.
The Author.
This first volume of the second Englished edition of Sobotta's Atlas of Descriptive Anatomy is translated and edited from the sixth German edition. Compared with the first Englished edition there are a number of differences, the chief one being that the text-book feature has disappeared, the book being more strictly an anatomical Atlas. The descriptions of the structures shown in the illustrations are greatly condensed and, as far as possible, are on the pages facing the illustrations under consideration. The labels on the figures are the B. N. A. terms in their original Latin form; in the text, however, it has seemed advisable to translate them, for the most part, into their English equivalents or, in rare cases, to use a term more familiar to English-speaking students. Where misunderstandings might occur the B.N.A. term in also given.
The text, however, is relatively unimportant; the illustrations are the chief glory of the book and to give these English explanations and to render them available for English-speaking students of anatomy is the object of this edition.
The Editor.
This second volume of the Atlas of Descriptive Anatomy treats of the anatomy of the viscera including the heart. It has seemed advantageous to include the heart since in dissection it is usually considered with the other viscera of the thorax.
The choice of preparations for illustration and their manner of representation follow the plan used in the first volume, the object being to present them from the standpoint of topographic anatomy.
Würzburg, August 1904.
The Author.
In this second edition a series of changes have been made in that the lithographic plates have been replaced by others, reproduced partly by so-called three-color printing partly by polychrome autotype printing. In so doing some plates were greatly altered and especially for the situs of the abdominal viscera and the peritoneum and partly for the female genitalia new figures have been added. All the figures are from the skilled hand of K. Hajek.
Würzburg, February 1914.
The Author.
In contrast to the third, fourth and fifth editions, which were essentially the same as the second, this sixth edition presents a number of new illustrations, especially of the stomach, intestines, liver, lungs and pericardium.
Bonn, November 1927.
The Author.
In this seventh edition all colored figures have been reproduced by the same method, i.e. by the polychromatic autotype process. Some additions have been made, of which there may be especially mentioned a series of new figures (mouth cavity, accessory cavities of the nose, thoracic viscera, conducting bundles of the heart). Further, some of the figures have been replaced by new ones.
Bonn, June 1931.
The Author.
An experience with the work of the Anatomical Laboratory, extending over many years, has convinced the author of the advisability of presenting illustrations of the peripheral nervous system and of the blood vessels as they are seen by the student in his dissections, i.e. the nerves and arteries of any region in the same figure. Consequently in the majority of the figures representing these structures arteries and nerves, arteries, veins and nerves, or arteries and veins are shown in each figure, and only occasionally is there a departure from this plan, when, for the sake of clearness, accessory figures showing only the arteries or the nerves (for example, the cranial nerves) are added.
This method of arrangement has the advantage for the student, that he finds on a single page of the Atlas representations of all the structures he has seen at any one stage of his dissection, and is not obliged to waste time in turning from page to page of the Volume. Each figure is one of a series of topographic anatomical illustrations.
The simultaneous representation of blood vessels and nerves makes reproduction in colors necessary. The arteries are shown red, the veins blue and the nerves yellow. For the reproduction in color autotypes have been used, prepared in a most satisfactory matter by Messers. Angerer and Göschl of Vienna and the various plates have at the same time been adapted for the coloration of the other tissues shown (muscles, bones, fat, skin etc.). In this way colored illustrations have been obtained, which do not, it is true, show an absolutely natural coloration, but nevertheless approximate it sufficiently to give an extraordinarily accurate general impression. All the figures of the Volume are from originals by K. Hajek, whose artistic talent and skill in anatomical illustrations are again fully manifested.
As was stated in the Preface to the first Volume, the endeavor has been to make of the Atlas a work that would be of use to students and practitioners, not one intended for expert Anatomists. Whoever wishes information in special fields of anatomy, will necessarily turn to special treatises on those fields, and this Atlas, even were it twice as extensive, would not be sufficient for him. On the other hand an undue expansion of the book and overloading it with illustrations of interest only to specialists, would only render it more difficult for the student or practitioner to get the information he desires. The chief object has therefore been to limit the illustrations to the necessities of the case, but to present these in a series of comprehensive figures, showing step by step the stages usually followed in dissection.
In correspondence with the arrangement followed in the first and second volumes, this one presents alternately pages of text and figures. The latter show the principal figures of the Atlas, the former, in addition to accessory and schematic figures and the explanations of the chief figures, a brief text intended for review during the use of the Atlas in the dissecting room, this being accompanied by references to other illustrations in the volume where the structures under consideration are shown.
Würzburg, May 1906.
The Author.
The Second Edition of this Atlas differs from the first by an increase in the number of illustrations. For the brain, especially, and for the sense-organs a number of new figures have been added. The representation of the principal fibre tracts has been extensively altered and in this connection some of the schematic figures have been replaced by new ones. In addition a considerable number of schemata have been added, which have in many cases been adapted from the admirable figures by Villiger.
The alphabetical index at the end of the Volume refers to the figures. In the text brief references are given to pages on which further statements as to the structures under consideration are to be found, and a special page reference was therefore unnecessary.
Würzburg, Spring, 1915.
The Author.
In contrast to the third, fourth and fifth editions, which were essentially the same as the second, this sixth edition presents a number of new illustrations, especially of the nerves and vessels of the lower limb, of the brain, the eye and the auditory organ.
Bonn, 1927.
The Author.
This seventh edition, compared with the sixth, has been improved, apart from lesser modifications, by the addition of three large, full-page, colored representations of the cranial, cervical and thoracic portions of the sympathetic nervous system, taken, by kind permission, from the admirable publications of Mr. Braeucker of Hamburg.
Bonn, November 1930.
The Author.
The eighth edition differs but little from the seventh, but contains some new illustrations of the blood vessels (and nerves), especially those of the posterior abdominal wall; and of the lymphatic vessels. Further the structure of the medulla oblongata, the pons and the corpora quadrigemina is shown in some schemata taken from the diagrams of Müller-Spatz, published by the J. F. Lehmann's Verlag.
Bonn, March 1933.
The Author.
Explanation of the abbreviations used in the illustrations.
Abbreviations not listed may be determined by the context.
X after a name denotes that the part indicated has been cut away or cut through.
( ) denotes that the part is seen through another structure. In the case of the facial muscles, however, ( ) denotes the proposed new nomenclature.
1, 2, 3, etc. after a term indicates that the part concerned is shown in different parts of its course.
If a part is not named, as a rule it has already been named on the preceding figure.
For the structure of bone see here.
The skeleton of the trunk consists of the vertebral column together with the ribs and sternum.
True and False Vertebrae may be distinguished. The former are represented by 7 cervical vertebrae, 12 thoracic and 5 lumbar, while the latter are two composite bones, the sacrum and coccyx.
The essential parts of a vertebra are the body (corpus), the arch (arcus), the transverse processes, the spinous process and the articular processes.
The body (Corpus) forms the principal part of the vertebra; it lies anteriorly and has a low cylindrical form. From it arises by means of the pedicles (radices) the arch (arcus), between which and the posterior surface of the body is the vertebral foramen, usually more or less transversely elliptical in form: Each pedicle (radix) presents an upper shallower and a lower deeper notch (incisura vertebralis). When the vertebrae are articulated the notches of successive vertebrae form foramina (foramina intervertebralia) through which the spinal nerves pass. Those vertebrae with which ribs articulate present toward the posterior part of both the upper and lower border of the body on each side an articular surface (fovea costalis superior and inferior) for the head of the rib.
The transverse processes are paired processes that project laterally from the anterior part of the arch or, in the case of the cervical vertebrae, from the pedicles. Their extremities, in the case of the thoracic vertebrae, present on their anterior surface an articular surface (fovea costalis transversalis) for the tubercle of the rib.
The unpaired, median spinous process arises from the posterior part of the arch and is directed backwards or backwards and downwards. The portion of the arch between the spinous and transverse process on each side is termed the lamina.
The paired articular processes serve for the articulation of the vertebrae with one another. Each vertebra bears two superior and two inferior articular processes. They arise from the arch close behind the pedicles and bear articular surfaces, which lie in different planes in different vertebrae.
The Cervical Vertebrae have small, transversely elliptical bodies, the upper concave surface of each overlapping laterally the lower convex surface of the vertebra next above. The arches are of moderate height and the vertebral foramen relatively large, especially in its transverse diameter, and of a rounded triangular form. The articulating processes have their almost flat surfaces situated obliquely in a plane intermediate between the frontal and the horizontal. The transverse processes enclose a foramen (foramen transversarium), the anterior portion of each process representing a rudimentary rib fused with the body and transverse process. The rib element of the seventh vertebra occasionally remains separate, forming a cervical rib. Each transverse process presents on its upper surface a groove for the spinal nerve (sulcus nervi spinalis), which extends from the vertebral foramen over the foramen transversarium to the tip of the process, where it separates an anterior from a posterior tubercle. This is due to the origin of the transverse processes from the pedicles, whence they lie in the regions of the vertebral incisures. The spinous processes are short and bifid at their tips; they are almost horizontal or only slightly inclined except that of the seventh vertebra (vertebra prominens), which inclines downwards like those of the thoracic vertebrae and is never bifid, resembling the spinous processes of the thoracic vertebrae rather than those of the other cervicals. On account of its long spinous process the seventh (vertebra prominens) is the first vertebra that can be felt in the living body. Furthermore its foramen transversarium is small. It is a typical cervical vertebra, presenting, however, characters transitional to those of the thoracic series.
The atlas and axis (epistropheus) are on the contrary atypical vertebrae. The atlas has no body. Instead there is both an anterior and a posterior arch. The vertebral incisures and the spinous process are also lacking. In place of the latter there is a posterior tubercle and opposite this on the anterior surface of the anterior arch there is ani anterior tubercle. In the place of the lacking articular processes there are articulating surfaces on the upper and under surfaces of what are termed the lateral masses of the bone. The large transverse processes have a foramen transversarium, but no tubercles and no groove for the spinal nerve. The posterior arch is low; on the posterior surface of the anterior arch is a roundish, slightly concave articular surface for the odontoid process (dens) of the axis (epistropheus). The vertebral foramen is very large and consists of a smaller anterior and a larger posterior portion; it is bounded laterally by the prominent lateral masses. Over the upper surface of the posterior arch there runs a shallow groove (sulcus arteriae vertebralis) for the vertebral artery; occasionally it becomes deeper or is even converted into a canal.
The axis (epistropheus) possesses a conical process, the odontoid process (dens) arising from its body. Upon this process there is an anterior and usually a posterior articular surface. The upper articular processes are replaced by articulating surfaces and the superior vertebral incisure is wanting. The transverse processes are very small; there are no tubercles and no groove for the spinal nerve. The spinous process is especially strong and bifid and it, as we)l as the under surface of the bone, resembles the corresponding part of typical cervical vertebrae.
The thoracic vertebrae have moderately large bodies which increase both in height and depth from above downwards. The surfaces of the bodies are flat and heart-shaped. The vertebral foramen is absolutely and relatively small and almost circular. On the posterior part of both the upper and lower borders of the lateral surfaces of the body are articular facets (fovea costalis superior and inferior) which, with the corresponding half facets of adjacent vertebrae, form the articular surfaces for the heads of the ribs. The articular processes have nearly flat surfaces which lie almost in the frontal plane; the lower ones hardly project beyond the surface of the arches. The transverse processes are strong, directed laterally and distinctly backward and bear upon the anterior surfaces of their thickened, free ends articular surfaces for the tubercles of the ribs (foveae costales transversales).
The spinous processes are very strong, triangular, thickened at their ends and directed distinctly downwards; those of the middle thoracic vertebrae overlap each other like the shingles on a roof.
The first thoracic vertebra has on each side a complete fovea for the first rib and a half fovea for the second rib, that is to say one and one half instead of two half foveae. The last two thoracic vertebrae have on each side a complete fovea, each articulating with only one rib. The eleventh and especially the twelfth thoracic vertebrae form a gradual transition to the lumbar vertebrae, since the spinous processes are directed straight backwards and are laterally compressed, the foveae costales transversales are lacking and, associated with a rudimentary condition of the transverse processes, accessory and mamillary processes may occur (12 Thoracic). Also the articular surfaces and the lower articulating processes of the twelfth thoracic vertebra are already sagittal in position.
The lumbar vertebrae are the largest of all the true vertebrae. They have high and broad bodies with flat, bean-shaped (that is to say, the contact surface for the adjacent vertebra is elliptical, but somewhat concave posteriorly) not quite parallel surfaces (the surfaces are not parallel because the lumbar portion of the vertebral column is strongly convex forwards, the vertebral bodies being noticeably higher in front than behind), as well as high and strong arches with very strong processes. The anterior as well as the lateral surfaces of the bodies are hollowed out (consequently the contact surfaces are larger than the transverse section through the middle of the bodies). In size these vertebrae increase continuously and quite distinctly from the first to the fifth. The vertebral foramen is narrow and rounded triangular. The surfaces of the articular processes stand almost in the sagittal plane; they are distinctly curved, the superior processes being concave and directed medially while the inferior are convex and directed laterally.
The upper articular processes bear on their upper margins a rounded tubercle, the mamillary process. The transverse processes are long, flat, rib-like and directed almost exactly laterally. At the base of each is a sharp process directed backwards, the accessory process, which corresponds to the tip of the transverse process of a thoracic vertebra, the main portion of a transverse process corresponding to a rib fused with the vertebra. The spinous processes are strongly compressed laterally, are directed almost exactly backwards and are slightly thickened at their ends.
The sacrum is a curved, shovel-shaped bone, broader above and narrower below. Its posterior surface (facies dorsalis) is convex and roughened, the anterior surface (facies pelvina) is concave and relatively smooth, the broader upper surface is termed the base and the lower more pointed end the apex.
The dorsal surface presents a rough median ridge or crest, which in many cases is frequently interrupted. It is formed by the fusion of the spinous processes of five sacral vertebrae. In addition to this unpaired median crest there are on the dorsal surface on each side two lateral, rarely continuous ridges, which are separated by four foramina, the posterior sacral foramina. Medial to these foramina lies the sacral articular crest formed by the fusion of the articular processes and lateral is a crest (crista sacral is lateralis) formed by the fusion of the transverse processes. The upper articular process of the first sacral vertebra remains distinct for articulation with the last lumbar vertebra, while the lower process of the last sacral vertebra forms a process, the sacral cornu, for articulation with the coccyx (but without an articular surface). The two sacral cornua bound the lower opening (hiatus sacralis) of the canal contained within the sacrum (canalis sacralis).
The pelvic surface presents four pairs of anterior sacral foramina corresponding to but larger than the four posterior foramina. Extending between the foramina of each pair is a low, rough ridge (linea transversa), which indicates the boundary between the bodies of two fused sacral vertebrae. The anterior foramina diminish in size from above downwards.
The apex of the sacrum appears as if cut off and possesses a small elliptical surface to which the coccyx is apposed.
The base shows a surface corresponding with the under surface of the last lumbar vertebra, with which it articulates. Between this bean-shaped surface and the superior articular process is a superior vertebral incisure, which, with the inferior incisure of the last lumbar vertebra, forms the last intervertebral foramen. Behind the surface for the last lumbar vertebra lies the upper end of the sacral canal and laterally are the lateral masses. The base of the sacrum is separated from the concave pelvic surface by a feeble line, which is the sacral part of the linea terminalis (see here).
In a lateral view of the sacrum one sees the articulating surface of the lateral mass, which serves for articulation on each side with the innominate bone and through this for the completion of the pelvic limb-girdle. It is formed anteriorly by an uneven, ear-shaped auricular surface, which is covered with cartilage, and posteriorly by a rough, depressed area, the sacral tuberosity, which is not covered by cartilage. Below this the lateral surface of the bone, which is fairly broad above, becomes exceedingly narrow; i.e. the bone which is relatively thick at the base now becomes quite thin.
The sacral canal, the continuation of the vertebral canal, traverses the entire length of the sacrum. Posteriorly it is bounded by a flattened bony mass formed by the fused arches of the sacrum, which bear the medial sacral crest. The canal opens in front and behind into the sacral foramina by means of the intervertebral foramina, which, in the sacrum, in contrast to the true vertebrae, are contained within the bone and consist of short canals. The posterior wall of the sacral canal does not extend to the apex of the bone, but terminates at about the boundary between the fourth and fifth sacral vertebrae. There is thus formed the hiatus of the sacral canal (see here).
The Coccyx is a small bone formed by the fusion of four or five rudimentary coccygeal vertebrae. The first of these vertebrae possesses two upwardly projecting cornua which are the rudiments of articular processes and serve for articulation with the sacrum. Furthermore, this same vertebra has feebly developed transverse processes. The upper end of the coccyx unites with the apex of the sacrum.
The second to the fifth (sixth) coccygeal vertebrae represent merely the bodies of these vertebrae and are usually irregular in shape, mostly flattened spherical. The individual coccygeal vertebrae are either united with one another by synchondroses or have a bony union (synostosis).
The vertebral column is a bony column with several curvatures and is composed of 26 separate bones, i.e. 24 true vertebrae, the sacrum and the coccyx. Its curvatures are as follows: One in the cervical region slightly convex anteriorly, one in the thoracic region strongly concave anteriorly, one in the lumbar region strongly convex anteriorly and one in the sacral and coccygeal regions strongly concave anteriorly. The transition from the lumbar convexity to the sacral concavity is somewhat abrupt; the region of the last intervertebral disc is termed the promontary.
The width of the column is greatest at the upper part of the sacrum; from this level the vertebrae become gradually smaller toward the coccyx and also upwards toward the middle of the thoracic region. From there upwards the vertebrae again broaden to the upper thoracic and lower cervical regions, diminishing again up to the axis (epistropheus), while the atlas, with its strongly developed transverse processes, is again notably broader. The greatest thickness of the column is in the lumbar region.
The bodies of the vertebrae are not in actual contact with one another, but are joined together by intervertebral discs. On the other hand the articular processes are in immediate contact by their articular surfaces. Each adjacent pair of vertebral incisures form an intervertebral foramen; the uppermost pair of these lies between the second and third cervical vertebrae and the lowest pair between the fifth lumbar vertebra and the sacrum, so that there are altogether 23 pairs of foramina. They are largest in the lumbar region and smallest in the thoracic. In the cervical region the foramina lie in the intervals between the transverse processes, in the thoracic and lumbar regions they are anterior to these processes.
The intervertebral foramina lead into the vertebral canal, which represents the sum of the separate vertebral foramina and is an almost cylindrical cavity that begins at the atlas and is continued below into the sacral canal (see here).
The ribs (costae) are long flat bones and may be regarded as consisting of a bony rib and a costal cartilage,. In the bony rib there may be noted a rounded enlargement at the posterior, vertebral end, the head (capitulum), with an articular surface for articulation with the vertebral bodies. This surface, at least in the ribs that articulate with the bodies of two vertebrae, is divided into two portions by the capitular crest. On the head there follows a distinct constriction of the rib, the neck (collum), whose upper border is provided with a ridge (crista colli) that gradually fades out on the body of the rib. Where the neck passes over into the body of the rib there is a rough tubercle bearing an articular surface for articulation with the transverse process of a thoracic vertebra.
The body (corpus) of the rib forms the principal part of the bony rib. It is a long, flat, vertically placed bone curved in correspondence with the curvature of the thorax. Near the tubercle it presents a rough surface, the angle of the rib, and at this point the rib, which at first was directed somewhat backwards, bends anteriorly. At the lower border, or more exactly, on the inner surface of the body, is a groove (sulcus costae), which gradually fades out toward the anterior end of the rib. This is slightly hollowed out for the reception of the costal cartilage.
The third to the tenth bony ribs have a typical form. The first and second and the eleventh and twelfth are atypical.
The first rib is short and broad. It is not placed vertically, but almost horizontally and its surfaces are directed upwards and somewhat outwards, and downwards and somewhat inwards. As a rule it has no capitular crest and no angle. On its upper surface, not far from where it joins its costal cartilage, there is a distinctly roughened area, the scalene tubercle for the insertion of the Scalenus anterior, and behind this a slight furrow, the subclavian groove for the subclavian artery. Behind this again is a rough surface for the insertion of the Scalenus medius. The neck of the first rib is long and thin.
The second rib is markedly longer and smaller than the first. Its posterior part is similar to that of the first, one surface looking upward and outward and the other downward and inward, but its anterior part is placed nearly vertical, as in the typical ribs. The angle and the tubercle coincide, but on the other hand there is a capitular crest. At about the middle of the length of the rib its lateral surface shows a roughened area, the tuberosity, for the insertion of a serration of the Serratus anterior.
The eleventh and twelfth ribs are quite rudimentary. They possess only a head, which however has no capitular crest. The tubercle is usually wanting on the eleventh rib and frequently the angle; on the twelfth rib also both are wanting. In both the costal sulcus is absent. The twelfth rib is often very short and it varies greatly in length.
The sternum is a flat, elongated bone in which three parts may be recognized, a manubrium, a body (corpus) and a xiphoid process.
The manubrium is the upper, broadest, slightly curved portion of the sternum and is separated from the body of the bone by the sternal synchondrosis. There may be distinguished on the manubrium an upper, shallow depression, the jugular notch or incisure, lateral to which on the two upper angles of the bone are two lateral, stronger depressions, the clavicular incisures, for the reception of the sternal ends of the clavicles. Immediately below these lie two broad shallow depressions, the first costal incisures, for the attachment of the cartilage of the first rib. At the lower end of the manubrium there is on either side a half incisure for the second rib.
The body (corpus) of the sternum is narrower and thinner but longer than the manubrium. For the most part it broadens from above downwards. It unites with the manubrium at a very obtuse angle, the sternal angle, which is not always very distinct. Its anterior surface is termed the sternal plane. The lateral borders show incisures for the reception of the second to the seventh costal cartilages. Frequently low transverse ridges upon the anterior surface of the bone unite the incisures of the two sides (see Fig. A39). Only the lower half of the incisure for the cartilage of the second rib is found on the body of the sternum, the incisures for the fifth to the seventh lie close to one another, while those for the second to the fifth rib are placed at quite distinct intervals. That for the seventh rib is in the angle between the body and the xiphoid process.
The xiphoid process is usually only partly bony, being usually cartilaginous in its lower part. It is often perforated or cleft below and is especially variable in form. Its upper bony portion usually fuses with the body of the sternum in advancing years.
The thorax is formed by the twelve thoracic vertebrae, the twelve pairs of ribs and the sternum.
The ribs increase in length from the first to the seventh and then diminish rapidly. The costal cartilages of the uppermost and lower-most ribs are the shortest.
The seven upper ribs which are attached by their cartilages directly to the sternum are termed the true ribs (costae verae), in contrast to the five lower ones, the false ribs (costae spuriae), which are attached to the sternum only through the intervention of the seventh costal cartilage, or, as in the case of the eleventh and twelfth ribs, have no connection with the other ribs or with each other (floating ribs). The cartilages of the sixth (in some cases even of the fifth) to the tenth rib are united with one another by upwardly and downwardly directed processes and form the costal arch. The union may be a synchondrotic one or else diarthrotic. In the region of the costal arch the cartilages are frequently greatly broadened. They always diminish in breadth from their outer ends towards the sternum. Not infrequently the middle ribs especially form what is termed a costal window, a rib dividing, usually in its bony portion, and then uniting again in the neighbourhood of the cartilage. The eleventh and twelfth ribs have only cartilaginous tips, which are very short and end freely.
The ribs, which form the principal part of the thoracic wall, are so placed that between each two ribs there is an interspace, the intercostal space, which is considerably wider than the rib itself. There are eleven of these spaces on each side. The last is very short and, like the next to the last, is open anteriorly.
The first and second costal cartilages slope slightly downwards toward the sternum, the third to the fifth are almost horizontal, while from the sixth downwards the cartilages are directed sharply upwards, especially in expiration, during which a distinct angle is developed at the junction of the bony rib with its cartilage, an angle which is almost completely obliterated during inspiration.
The sternum with the costal cartilages and the adjacent portions of the bony ribs forms the anterior wall of the thorax. It does not lie exactly in the frontal plane, but its upper end is directed somewhat backwards and is therefore somewhat nearer the vertebral column than is the lower part. The greater distance of the lower part from the column is mainly due to the strong concavity of the thoracic portion of the column.
The anterior wall of the thorax is markedly shorter than the posterior, since the upper border of the manubrium sterni corresponds to the interval between the second and third thoracic vertebrae in the neutral position, being lower during expiration and higher in inspiration. The tip of the xiphoid process lies at the level of the ninth thoracic vertebra, or, in accordance with its variable length, occasionally at that of the eighth or tenth.
The posterior wall of the thorax is formed by the twelve thoracic vertebrae and the posterior portions of the twelve pair of ribs. Since the bodies of the former project strongly into the thoracic cavity there is a deep groove on each side of the vertebral column, the pulmonary groove (sulcus pulmonalis).
The lateral wall of the thorax is formed by the bony ribs. It is longer posteriorly than in front, where the eleventh and twelfth ribs are lacking, and during expiration reaches, opposite the twelfth rib, the level of the second lumbar vertebra.
The walls of the thorax enclose the thoracic cavity, which is almost conical in shape, the apex being directed upwards. This cavity has an upper and a lower aperture, the upper one being markedly smaller than the lower. It is bounded by the first thoracic vertebra, the first rib and the upper border of the manubrium sterni. The much larger lower aperture is bounded by the twelfth thoracic vertebra, the twelfth, eleventh and tenth ribs, the costal arch and the xiphoid process. The angle that the costal arch forms with the xiphoid process is known as the infrasternal angle.
In transverse section the thoracic cavity is heart-shaped or kidney-shaped on account of the manner in which the bodies of the vertebrae project into it. As a result the sagittal diameter of the thorax is small, much smaller than the transverse, especially in the upper part.
The bones of the head taken together form what is termed the skull (cranium). Two groups of skull bones are usually recognized, the bones of the cranium and the bones of the face. To the former belong the occipital, the sphenoid, the temporals, the parietals, the frontal and the ethmoid.
The bones of the face are the nasals, the lacrimals, the vomer, the inferior concha, the maxillae, the palatines, the zygomatics, the mandible and the hyoid.
In the occipital bone the following parts may be distinguished:
The basilar portion lies in front of the foramen magnum, the lateral portions form the lateral boundaries of this and the squamous portion lies behind it.
The basilar portion in the skull of the adult is continuous at its anterior end with the body of the sphenoid. It presents a horizontal, roughened, lower surface, which has in the median line a tubercle, the pharyngeal tubercle. Its upper or cerebral surface is concave. This latter surface forms the larger and posterior part of the clivus and shows a shallow groove at the margin of the petro-occipital fissure, the inferior petrosal groove.
The lateral portions bear upon their under surfaces the elongated, convex occipital condyles and pass without any sharp boundary into the basilar portion anteriorly and the squamous portion posteriorly. Behind the condyles is a shallow depression, the condyloid fossa, in which a short condyloid canal usually opens. When this canal is present its inner opening is on or near a broad groove, the sigmoid sulcus (Fig. A56). This, on the cerebral surface of the lateral portion, arches around the jugular process, beginning at the jugular notch, which, together with a similar notch on the temporal bone forms the jugular foramen. A small projection (intrajugular process) on each of these two bones divides the foramen into a small anterior (medial) and a larger posterior (lateral) portion (Fig. A55). The jugular process projects strongly laterally and serves for the articulation of the lateral portion of the occipital with the pyramid of the temporal bone. Medial to the jugular process. There is on the cerebral surface of the lateral portion a rounded elevation, the jugular tubercle (Fig. A56). Between this and the condyle there passes almost transversely through the bone the hypoglossal canal for the nerve of that name.
The squamous portion is by far the largest portion of the occipital bone. It is rather flat but is curved like a shovel, being concave on the inner surface and convex on the outer. It is typically triangular. Along the occipito-mastoid suture it articulates with the mastoid portion of the temporal bone and at the lambdoid suture with the two parietal bones. The upper angle abuts in the middle of the lambdoid suture upon the posterior end of the sagittal suture. Its cerebral surface presents a cross-like figure, whose upper and lateral arms are formed by grooves, while the lower arm is formed by a ridge, the internal occipital crest, which passes toward the posterior border of the foramen magnum. The groove forming the upper arm of the cross is the lower portion of the sagittal sulcus, while the transverse grooves are the transverse sulci; the similarly named blood sinuses of the dura mater occupy these sulci. The central point of the cross-like figure is the internal occipital protuberance. The arms of the cross-like figure separate two shallow superior occipital fossae from one another and from two deeper inferior occipital fossae.
The outer surface of the squamous portion of the occipital is divided into two parts by the superior nuchal lines, which pass laterally from the external occipital protuberance. The upper, triangular, relatively smooth part is the occipital surface, the lower rough part the nuchal surface. Above the superior nuchal lines there are usually two arched supreme nuchal lines. From the external occipital protuberance the external occipital crest extends downwards toward the posterior border of the foramen magnum, and from about its middle the inferior nuchal lines curve outwards, parallel to the superior ones.
The sphenoid bone has an unpaired body (corpus), two great wings (alae magnae), two lesser wings (alae parvae) and two pterygoid processes.
The body (corpus) unites in later life by its posterior surface with the basilar portion of the occipital. It contains a cavity filled with air, the sphenoidal sinus, which is divided into two parts by a septum and communicates by two apertures with the posterior part of the nasal cavity. The septum shows itself on the anterior surface of the body as the sphenoidal crest. The anterior wall is formed by two thin bony plates, the sphenoidal conchae, which originally belong to and are often united with the ethmoid bone. The sphenoidal crest is continued upon the under surface of the body as the rostrum and serves for articulation with the wings of the vomer. The upper surface of the body is partly formed by the sella turcica, in front of which is a flat surface, which posteriorly bounds the sulcus chiasmatis of the sella turcica and anteriorly projects towards the lamina cribrosa as the ethmoidal spine. The posterior boundary of the sella turcica is the dorsum sellae with the two posterior clinoid processes at its outer ends; in front of it is the deepest part of the sella, the hypophyseal fossa, which is bounded in front by the tuberculum sellae (Fig. A48). In front of the tuberculum sellae there is a shallow, transverse groove, the sulcus chiasmatis. From the lateral parts of the tuberculum sellae the short middle clinoid processes project. At the sides of the hypophyseal fossa and on the root of the great wing there is a shallow, but broad, longitudinal groove, the carotid groove, for the internal carotid artery. It is bounded laterally by a small bony plate, the sphenoidal lingula (Fig. A48). The anterior part of the clivus, behind the dorsum sellae, belongs to the sphenoid bone (Fig. A48).
The lesser wings (alae parvae) are small horizontal plates of bone which arise from the lateral surfaces of the body of the sphenoid, each by two roots which enclose the optic foramen. Their anterior borders articulate with the orbital portion of the frontal bone in the spheno-frontal suture; their posterior sharper borders form a boundary for the anterior and middle cranial fossae and end medially, toward the sella turcica, in sharp hook-like points, the anterior clinoid processes. The lesser and greater wings are completely separated by the superior orbital fissures.
The great wing (ala magna) arises from the lateral surface of the body of the sphenoid. In its root there are three foramina, the foramen rotundum directed obliquely forward and leading into the pterygopalatine fossa, the elliptical foramen ovale also placed obliquely and the small, round foramen spinosum. The great wing has three principal surfaces, cerebral, temporal and orbital, and the following borders, a squamous border (margo squamosus) for the squamous portion of the temporal, a frontal border (margo frontalis) for the orbital portion of the frontal, a zygomatic border (margo zygomaticus) for the zygomatic and a parietal angle for the parietal. The lateral posterior process which bears the external opening of the foramen spinosum and is directed toward the under surface of the pyramid of the temporal bone is termed the spine of the sphenoid (spina angularis). The cerebral surface is concave and, in addition to the three foramina, shows digitate impressions. The orbital surface is almost flat and forms a part of the lateral wall of the orbit. A sharp orbital crest separates it from the small spheno-maxillary surface. Similarly the temporal surface is divided by the infratemporal crest into the upper temporal and the lower infratemporal surfaces, the latter, again, passing into the spheno-maxillary surface, there being frequently between the two a sphenomaxillary crest. The infratemporal surface bears the external openings of the foramen ovale and foramen spinosum, the spheno-maxillary surface that of the foramen rotundum.
The pterygoid processes extend almost vertically downwards, almost parallel with one another, from the under surface of the body of the sphenoid; they arise on each side by two roots which enclose between them the pterygoid(Vidian) canal, which is directed almost horizontally in the sagittal plane. It unites the foramen lacerum with the pterygo-palatine fossa. Below, the pterygoid processes divide into a smaller inner and a broader outer plate (lamina) separated in their upper part by a groove, the pterygoid fossa, in their lower part by a cleft, the pterygoid fissure, which is filled by the pyramidal process of the palatine bone. The inner plate has at its base an elongated shallow depression, the scaphoid fossa, and at its lower end and separated from it by a groove, the hamulus. A small process projecting toward the body of the sphenoid, the processus vaginalis, encloses the pharyngeal canal by uniting with a process of the palatine bone. From the scaphoid fossa a shallow groove, sulcus tubae auditivae extends toward the spinous process along the spheno-petrous suture. On the anterior surface of the pterygoid process is a groove, the pterygo-palatine groove, extending downwards from the anterior opening of the pterygoid canal. It forms with the corresponding grooves on the palatine bone and maxilla the pterygo-palatine canal.
The temporal bone has four parts:
These four parts group themselves around the external auditory opening, in such a way that the squamous part lies above it, the mastoid part behind, the tympanic part below and anterior, and the petrous part medial and anterior.
The squamous portion (squama temporalis) articulates by a strongly curved, irregular border with the great wing of the sphenoid (margo sphenoidalis) and with the parietal (margo parietalis), the margins of the temporal bone overlapping those of the other hones in a squamous suture. Except for a small lower portion the squama is vertical in position and has an outer temporal and inner cerebral surface, the latter having ridges and depressions for the convolutions of the cerebral hemispheres and also grooves for the middle meningeal artery. It is more or less separated from the petrous portion by a petro-squamosal fissure, which tends to become obliterated in the adult. The temporal surface is smooth and presents a shallow groove for the middle temporal artery, beginning just above the external auditory opening. In addition there arises from the temporal surface the long zygomatic process, which articulates with the temporal process of the zygomatic bone. The process arises by a root from the vertical portion of the squama and by a second root from the small, lower, horizontal portion. Between the two roots lies the articular cavity for the head of the mandible (fossa mandibularis), in front of which is an articular tubercle, also partly covered with cartilage. The zygomatic process is at first almost horizontal, but later twists so as to lie in the sagittal plane. From its posterior extremity the hinder part of the temporal line passes upwards and backwards to be continued upon the parietal bone. Above the external auditory opening there is usually a sharp projection, the suprameatal spine.
The mastoid portion has as its chief part the large mastoid process, which forms the whole outer surface of this portion of the bone; it articulates by the parietal notch with the mastoid angle of the parietal and by its occipital margin with the squamous portion of the occipital (occipito-mastoid suture). It possesses a concave inner (cerebral) surface and a strongly convex roughened outer surface. The latter forms the broad, conical mastoid process which contains cavities filled with air, the mastoid cells, which communicate with the tympanic cavity. It gives attachment to several muscles and towards its posterior border has a deep groove (mastoid incisure) for the Digastric. Near the occipito-mastoid suture is a shallow groove for the occipital artery and the external opening of the mastoid foramen.
The principal part of the temporal bone, the petrous portion, is also termed the pyramid and is a three-sided pyramidal structure lying almost horizontally. In the adult only its three surfaces can be seen, the base being almost covered by the tympanic portion of the bone; in the new-born child and even somewhat later it is visible on the outer surface of the bone (Fig. A64, A65). The schematic sections (Fig. A66 and A67) show the arrangement of the four surfaces as well as the formation of the tympanic cavity and its continuation as the Eustachian tube (musculo-tubar canal) through the petrous and tympanic portions.
In the description that follows the parts of the bony labyrinth lying within the pyramid are not considered, nor is the tympanic cavity fully described. These parts will be described later (see here).
Two surfaces of the petrous portion, the anterior and the posterior, look toward the skull cavity; the third, inferior, is at the base of the skull, while the base (not labelled) forms the medial wall of the tympanic cavity. The three surface are separated by angles; the superior angle separates the anterior and posterior surfaces, the anterior separates the anterior and inferior and the posterior the posterior and inferior surfaces. The axis of the pyramid is oblique to the long axis of the skull passing from behind and lateral, anteriorly and medially. The apex of the pyramid lies at the foramen lacerum.
The anterior surface forms a portion of the middle fossa of the skull. It is separated by the petrosquamous fissure from the squamous portion of the bone, and bears a slight transverse elevation, the arcuate eminence, which is formed by the underlying semicircular canal.
Further towards the median line is a slit-like opening the hiatus of the facial canal, with a groove for the great superficial petrosal nerve extending toward the foramen lacerum.
Lateral and anterior to this is a second opening, the aperture of the superior tympanic canaliculus, with a similarly directed groove for the lesser superficial petrosal nerve. The part of the anterior surface of the pyramid that lies between the petro-squamous fissure and the arcuate eminence forms the roof of the tympanic cavity, the tegmen tympani. Near the apex of the pyramid is a very shallow trigeminal impression (see Fig. A48). The superior angle bears the superior petrosal groove and the anterior angle bounds the spheno-petrous fissure and the foramen lacerum. The posterior surface of the pyramid forms a part of the posterior cranial fossa. It presents a roundish opening, the internal auditory opening (porus acusticus internus), which leads into a canal, the meatus acusticus internus, running obliquely into the bone. Above this opening, immediately below the superior angle, is small depression, the subarcuate fossa, and lateral to the auditory opening there is a fissure-like opening, the external opening of the aquaeductus vestibuli, which lodges a portion of the internal ear. A shallow groove, the inferior petrosal sulcus, runs parallel to the posterior angle, being a continuation of the similarly named groove on the occipital bone. The apex of the pyramid has an opening with an irregular boundary, the internal carotid foramen (see below). Beside it, near the anterior angle of the pyramid, is the opening of a large canal, the Eustachian canal (canalis musculo-tubarius), which leads into the tympanic cavity.
The posterior angle is separated from the occipital bone by- the petro-occipital fissure and bears a shallow jugular notch, which, with the corresponding notch on the occipital forms the jugular foramen (see Fig. A48).
The inferior surface of the pyramid presents the stylomastoid foramen at the base of the mastoid process; it is the outer opening of the facial canal. In front of it lies the slender, often very long styloid process, whose base is partly ensheathed by a plate-like projection of the tympanic portion, the vaginal process. Close to the styloid process is a broad, elongated groove, the jugular fossa, which abuts medially upon the jugular notch and receives the bulb of the jugular vein. In the floor of the groove is the small sulcus of the mastoid canaliculus. On the posterior margin close to the jugular fossa is a small opening, the external aperture of the cochlear canaliculus; in front of this is the large round external carotid foramen and between this and the jugular fossa is a small depression, the petrous fossula, from which a small canal, the tympanic canaliculus, passes through the floor of the tympanic cavity.
The base of the petrous portion forms the medial wall of the tympanic cavity. In the adult it is covered in by the tympanic portion of the bone, so that only a small strip of it is visible at the surface along the petro-tympanic fissure.
The tympanic cavity is an air-containing cavity lying between the petrous and the tympanic portions. The external auditory meatus leads into it from without; its roof is formed by a thin part of the petrous portion, the tegmen tympani, while its floor is formed partly by the petrous and partly by the tympanic portion. Anteriorly and medially the cavity is continued into the canal for the Eustachian tube (canalis musculo-tubarius) and posteriorly and laterally it has opening into it the antrum and the mastoid cells. It contains the three small auditory ossicles, which together with the walls of the cavity will be described in connection with the auditory organ (see here).
The tympanic portion of the temporal bone is a small trough-shaped plate of bone which forms the sides and floor of the external auditory meatus and the lateral wall of the tympanic cavity. It is separated from the petrous and squamous portions by the petro-tympanic fissure (fissure of Glaser), from the mastoid portion by the tympano-mastoid fissure and it forms the vagina of the styloid process.
The temporal bone of the new-born child differs markedly from that of the adult in that the tympanic portion has the form of a ring that is open above, and there is practically no mastoid process. The squamoso-mastoid suture is still quite distinct, separating the squamous portion from the mastoid and petrous portions, which form a single mass. In the course of the first year the tympanic ring becomes the trough-like structure, which at first has in its floor a constant foramen.
The facial canal, mainly for the facial nerve, begins at the bottom of the internal auditory meatus and runs at first horizontally and almost transversely to the axis of the petrous portion to the hiatus of the facial canal. There it bends at a right angle and runs in the medial wall of the tympanic cavity, again almost horizontally, but in the line of the axis of the pyramid, until it reaches the pyramidal eminence of the tympanic antrum (see here). Here it bends to assume a vertical direction and opens by the stylomastoid foramen. From the lower portion of the canal the canaliculus for the chorda, tympani leads to the tympanic cavity.
The carotid canal is a short, but wide canal, situated near the apex of the pyramid. It begins at the external carotid foramen and runs at first vertically, but later bends almost at a right angle so as to run horizontally, and ends at the internal carotid foramen. Small canals, the carotico-tympanic canaliculi, lead from it into the tympanic cavity.
The canal for the Eustachian tube (canalis musculo-tubarius) runs parallel with and immediately adjacent to the horizontal portion of the carotid canal, almost in the axis of the pyramid. It begins as a notch on the anterior angle of the pyramid, between that part of the bone and the squamous portion, and ends on the anterior wall of the tympanic cavity of which it seems to be a direct prolongation. An incomplete horizontal septum divides it into an upper canal for the Tensor tympani and a lower one for the Eustachian tube (tuba auditiva).
The tympanic canaliculus leads from the petrous fossula into the tympanic cavity, where it becomes the sulcus promontorii, and then leaves the cavity by its upper wall to open by the superior aperture of the tympanic canaliculus on the anterior surface of the pyramid.
The very narrow mastoid canaliculus begins as a groove in the jugular fossa, passes through the lower portion of the facial canal and opens in the tympano-mastoid fissure.
The parietal bone is large quadrangular flat bone, convex on its outer surface and concave on its inner. The four borders are
The four angles of the bone are the frontal situated at the junction of the sagittal and coronal sutures, the occipital at the junction of the sagittal and lambdoid sutures, the mastoid at the parieto-mastoid suture, where it occupies the parietal notch of the temporal bone, and the sphenoidal which articulates in the spheno-parietal suture with the great wing of the sphenoid. This last angle is the sharpest.
The outer convex surface presents at the region of greatest curvature the tuberosity and also stronger superior and weaker inferior temporal lines, both of which have an arched course. Below the latter line the parietal forms a part of the temporal surface (see Fig. A44, A45). In this region the squamosal border is rough, being overlapped by the squamous portion of the temporal bone. Near the posterior end of the sagittal border and close to the sagittal suture is the parietal foramen.
The inner (cerebral) surface shows well marked arterial grooves, especially on the anterior part of the bone, produced by the branches of the middle meningeal artery. At the sagittal border there is the one half of the sagittal sulcus and at the mastoid angle one sees a short portion of the sigmoid sulcus. Not infrequently the cerebral surface presents digitate impressions and juga cerebralia and frequently also Pacchionian depressions (foveolae granulares) which may be of considerable depth, especially in middle and old age.
The frontal bone consists of two unpaired portions, the frontal plate and the nasal portion, while the orbital portions are paired.
The frontal plate forms the principal part of the bone. It articulates by its parietal border with both parietals in the coronal suture and by its sphenoid border with the great wing of the sphenoid in the spheno-frontal suture. The outer surface is strongly convex and presents at the middle of each half the tuber frontale. Above the margins of the orbits are two arched projections, the supraciliary arches, and between these the somewhat depressed glabella. The upper border of the orbit separates the frontal plate from the orbital portion. Its lateral part is formed by the zygomatic process which unites with the fronto-sphenoidal process of the zygomatic bone in the zygomatico-frontal suture. From the zygomatic process the temporal line takes origin and separates from the frontal surface a small almost vertical portion, the temporal surface. In the inner half of the supraorbital border are two notches, the medial frontal notch and the lateral supraorbital notch, this latter being frequently converted into a foramen, the supraorbital foramen.
The cerebral surface of the frontal plate possesses in its lower portion a median ridge, the frontal crest. This begins below at a foramen, the foramen caecum, bounded by the frontal arid ethmoid bones in common, and running upwards into the sagittal sulcus. The surface is smooth, except. for some digitate impressions and juga cerebralia, as well as Pacchionian depressions (foveolae granulares). It passes over without sharp demarcation into the cerebral surface of the orbital portion.
The orbital portions are separated from one another by a deep ethmoidal notch which receives the lamina cribrosa of the ethmoid. Each possesses an upper cerebral and a lower orbital surface. The former shows very abundant digitate impressions; the latter is concave and forms the roof of the orbital cavity. It presents on its medial portion a small depression, the fovea trochlearis (occasionally also a trochlear spine), and on its lateral part a shallow depression, the lacrimal fossa, for the lacrimal gland. The borders of the ethmoidal notch are broad and rough since they bear the ethmoidal foveolae, which complete the ethmoidal cells. Furthermore they bear an anterior and posterior groove (or short canal), which serve to form the anterior and posterior ethmoidal foramina.
The nasal portion of the frontal is the small, median part that unites the two supraorbital margins. It has an irregular, rough surface, for articulation with the nasal bones and the frontal processes of the maxilla and, in addition, the frontal spine, directed downwards and serving for the fixation of the bones that form the skeleton of the nose. Near the spine lie the openings of the frontal sinus, which is divided into two parts by a septum. Above the spine on the outer surface of the bone is a smooth flattened area, the glabella.
The ethmoid is an irregular, cubical bone in which a middle unpaired and two lateral paired portions may be distinguished. The middle portion consists of a horizontal plate, the lamina cribrosa, and a vertical plate, the lamina perpendicularis. The paired lateral portions are attached to the lateral edges of the lamina cribrosa and are known as the ethmoidal labyrinths.
The lamina cribrosa occupies the ethmoidal notch of the frontal bone and is a rectangular plate situated between the nasal and cranial cavities. It is perforated by a number of roundish foramina, through which the branches of the olfactory nerve pass to the nasal cavity. At its middle it bears a -thick ridge, high in front and diminishing posteriorly, the crista galli. In front of this are two small processes of the lamina cribrosa, the alar processes, which usually assist in the boundary of the foramen caecum.
The lamina perpendicularis is a thin pentagonal plate which forms the upper anterior part of the nasal septum. It is attached by its anterior, upper border to the frontal spine of the frontal, by its upper border it is fused with the lamina cribrosa, by its posterior border it articulates with the sphenoidal crest, by its lower border with the upper border of the vomer and by its anterior lower border with the cartilaginous nasal septum (see also Fig. A82).
The ethmoidal labyrinth hangs almost vertically downwards from the lateral border of the lamina cribrosa. It contains numerous, air-containing, imperfectly separated spaces, the ethmoidal cells, which in part are completely in the ethmoid itself, but for the most part are also bounded by other bones, the maxilla, lacrimal, frontal, sphenoid and palatine. The lateral wall of the labyrinth, by its thin lamina papyracea, forms a part of the medial orbital wall. Upon it or in the suture between it and the orbital portion of the frontal lie the anterior and posterior ethmoidal foramina.
The medial wall of the ethmoidal labyrinth forms the greater part of the lateral wall of the nasal cavity. It possesses two parallel projections, having the form of thin plates, curved upon themselves at their lower border, the nasal conchae. The superior concha is markedly smaller and shorter than the middle (see here). The latter projects beyond the labyrinth both anteriorly and posteriorly and is attached by its ends to the ethmoidal crests of the maxilla and palatine bones. It sends downwards a hook shaped processus uncinatus, which partly covers the opening of the maxillary sinus (see here and Fig. A88).
The vomer is a flat, quadrangular bone which forms the lower and posterior portion of the nasal septum. Its upper end is thickened and cleft into two alae, which enclose the rostrum of the sphenoid. The small anterior border articulates with the cartilaginous part of the nasal septum, the upper border with the lower border of the lamina perpendicularis of the ethmoid, the lower border with the nasal crest of the maxilla and palatine and the posterior border forms the septum of the choanae.
The maxilla is a paired bone which takes part in the boundaries of the orbital, nasal and oral cavities. In it may be distinguished the body (corpus) and four processes. The body is irregularly cubical and encloses a large air-containing cavity, the maxillary antrum or sinus, which communicates by a wide opening with the nasal cavity. The body has four surfaces. The anterior is the facial surface and is convex; its upper infraorbital border forms part of the lower border of the orbit, below which is the infraorbital foramen, the opening of the infraorbital canal, and below this a shallow depression, the canine fossa. The orbital surface is triangular and forms the greater part of the floor of the orbit, bounding the inferior orbital fissure medially. It possesses a groove, the infraorbital groove, which gradually becomes converted into a canal. The lacrimal notch near the root of the frontal process, receives the hamulus of the lacrimal bone. The infratemporal surface is the posterior surface and forms the boundaries of the infratemporal and pterygopalatine fossae. The swollen end of this portion of the bone is termed the tuberosity; it presents several small alveolar foramina and also a pterygo-palatine groove, which completes the canal of the same name (see here).
The nasal surface forms the lower part of the lateral wall of the nasal cavity, but in its posterior portion it is covered in by the posterior part of the perpendicular portion of the palatine bone. It presents the wide irregular opening of the maxillary sinus, in front of which is a broad groove, the lacrimal groove (see below), and at the junction of the nasal surface with the frontal process the horizontal conchal crest (see below).
The frontal process of the maxilla is directed upwards and articulates by its upper border with the nasal portion of the frontal bone in the fronto-maxillary suture, by its lacrimal border with the lacrimal bone and by its medial border with the nasal bone.
It presents an outer and inner surface; the latter forms part of the lateral wall of the nasal cavity and bears an ethmoidal crest for articulation with the anterior part of the middle concha and below this a conchal crest for the inferior concha. Behind the process is the broad lacrimal groove, which, with a similar groove on the lacrimal bone forms the fossa for the lacrimal sac. The anterior wall of the groove is termed the anterior lacrimal crest. The zygomatic process is a broad, short, triangular process, projecting laterally to articulate with the zygomatic bone in the zygomatico-maxillary suture. The alveolar process is convex externally and concave on its inner surface, passing without distinct demarcation into the body on the one side and the palatine process on the other. The processes of the two maxillae meet in the intermaxillary suture, which ends anteriorly in the anterior nasal spine. The alveolar process forms the lateral and lower boundary of the piriform aperture. Its lower border is the alveolar border (limbus alveolaris) and bears the sockets for eight teeth, separated by interalveolar septa. The anterior surface of the process usually shows juga alveolaria, corresponding to the roots of the anterior teeth. The palatine process forms the greater portion of the hard palate and projects medially from the inner surface of the body. It is rough and uneven on its oral surface, smooth and concave on its nasal surface. The two processes unite by thickened borders to form the anterior part of the median palatine suture, which, on the nasal surface, forms the nasal crest. Anteriorly in the line of the suture is the incisive canal, which begins in an incisive notch on each maxilla and terminates on the nasal surface in two incisive foramina one on either side of the nasal crest.
The lacrimal bone is a very thin, flat, quadrangular bone that lies in the medial wall of the orbit between the frontal process of the maxilla and the lamina papyracea of the ethmoid. It presents orbital and ethmoidal surfaces. The latter closes certain of the ethmoidal cells and articulates on the lateral wall of the nasal cavity with the lacrimal process of the inferior concha. The former presents anteriorly the lacrimal groove, which is bounded posteriorly by the posterior lacrimal crest. This ridge runs downwards and terminates in a hook-like process, the hamulus, which fits into the lacrimal notch of the maxilla. Behind the ridge the orbital surface of the lacrimal forms a part of the medial wall of the orbit.
The inferior concha is a small, thin, porous bone whose free medial border is curled on itself, while the lateral border is attached to the conchal crests of the maxilla and palatine bone. It has three processes; the maxillary process extends downwards and laterally to the maxilla and closes a considerable portion of the opening of the maxillary sinus; the lacrimal process ascends to the lacrimal bone and forms a part of the posterior wall of the nasolacrimal canal; the ethmoidal process articulates with the uncinate process of the ethmoid, anterior to the opening of the maxillary sinus.
The palatine bone is a flat bone formed of two plates arranged at right angles to one another; one is the horizontal portion and the other the perpendicular portion. The horizontal portions of the two bones form the posterior part of the hard palate and resemble in every particular the palatine processes of the maxilla, from which they are separated by the transverse palatine suture. At the hinder end of the median palatine suture they form the posterior nasal spine and enclose on each side the greater palatine foramen, the inferior opening of the pterygopalatine canal.
The perpendicular portion is narrower, but longer than the horizontal. Its maxillary surface overlies the posterior part of the nasal surface of the maxilla, while its nasal surface forms a part of the lateral wall of the nasal cavity. It bears two parallel, horizontal ridges, a lower stronger conchal crest for the inferior and an upper ethmoidal crest for the middle concha. Posteriorly it articulates with the pterygoid process of the sphenoid, its posterior border showing a furrow, the pterygo-palatine groove, which, with corresponding grooves on the pterygoid process and maxilla, forms the pterygo-palatine canal.
Three processes of the palatine bone are recognized. The pyramidal process is directed backwards and is short and broad. It fits into the pterygoid notch of the pterygoid process, completing the pterygoid fossa. It usually presents the posterior openings of the lesser palatine foramina. The orbital and sphenoidal processes arise from the upper border of the perpendicular portion and are separated by the spheno-palatine notch. The larger orbital process looks laterally and anteriorly, forms a small part of the floor of the orbit and articulates with the lamina papyracea of the ethmoid in the palato-ethmoidal suture and with the maxilla in the palato-maxillary suture, closing along these sutures the adjacent ethmoidal cells. The sphenoidal process is directed medially and posteriorly and articulates with the under surface of the body of the sphenoid. In addition the perpendicular portion gives origin at its base to a variable, but constant, process, the maxillary process. It is crescentic in shape and closes in, according to its size, a greater or less portion of the opening of the maxillary sinus, coming into relation with the maxillary process of the inferior concha (Fig. A90).
The nasal bones form a part of the bony arch of the nose. They are small, flat, oblong bones, separated from each other by the internasal suture. They have a shorter medial and a longer lateral border, the latter articulating with the frontal process of the maxilla in the naso-maxillary suture. The upper and lower borders are irregular; the former articulates with the nasal portion of the frontal, the latter with the nasal cartilage. The posterior surface presents an ethmoidal groove, from which one or several nasal foramina pass to the outer surface of the bone.
The zygomatic (malar) bone is a rather thick triangular bone. Of its three surfaces the malar forms part of the face and is convex; it passes over into the zygomatic process of the maxilla and presents a zygomatico- facial foramen. The orbital surface is slightly concave and forms part of the lateral wall of the orbit; in half the cases it is a boundary of the anterior part of the inferior orbital fissure and presents one or two zygomatico-orbital foramina. The temporal surface is concave and presents the zygomatico-temporal foramen.
The bone has two processes. The temporal process projects horizontally backwards and articulates with the zygomatic process of the temporal to form the zygomatic arch (zygoma). The fronto-sphenoidal process- is directed upwards to form part of the lateral wall of the orbit and articulates with the zygomatic process of the frontal and with the zygomatic border of the great wing of the sphenoid.
In the mandible there may be recognized a body (corpus) and two rami. The body is a thick curved plate from the posterior part of which the rami extend upwards almost at right angles.
The lower part of the mandible is termed the base and the tooth-bearing part the alveolar portion. The free border of the latter is termed the limbus alveolaris and bears the dental alveoli, separated from one another by interalveolar septa; it also presents juga alveolaria corresponding to the roots of the teeth. The outer surface of the body has in the middle line a roughened flat ridge, the mandibular protuberance, and lateral to this on the base on each side is a mental tubercle and further laterally the mental foramen, the anterior opening of the mandibular canal which traverses the bone. In addition there passes downwards upon the body from the anterior border of the ramus a smooth ridge which gradually diminishes in height and is termed the oblique line.
The inner surface of the body shows close to the middle line on each side a shallow digastric fossa, and between the two fossae and somewhat higher a sharp prominence, often doubled, the mental spine. Lateral to this is a distinct depression, the sublingual fovea for the sublingual gland and more laterally a much shallower, frequently indistinct, depression, the submaxillary fovea for the submaxillary gland. A rough line, beginning on the inner surface of each ramus, runs downwards and forwards upon the body, gradually becoming less distinct; it is the mylohyoid line and below it is a groove which extends downwards and forwards from the mandibular foramen, the mylohyoid groove.
Each ramus presents a medial surface, turned towards the oral cavity, and a lateral surface. Its lower posterior angle is termed the angle of the mandible. At about the middle of the medial surface is the mandibular foramen, which has a somewhat oblique position and opens into the mandibular canal; its inner border is raised into a projecting spine, the lingula. Above, each ramus divides into two processes separated by the mandibular notch. The anterior is the coronoid process, which is transversely flattened and sharp at its extremity; from its base a ridge, the bucinator ridge, extends to the neighbourhood of the last molar tooth. The posterior process is the condyloid process.
On the lateral surface of the angle of the mandible is the masseteric tuberosity and opposite it, on the medial surface, the pterygoid tuberosity for the attachment of similarly named muscles.
The condyloid process, situated posterior to the mandibular notch, bears at its upper end a head (capitulum) with an articular surface for the mandibular fossa of the temporal bone. It has the shape of an almost transversely directed cylinder. The constriction below the head is termed the neck (collum) and a depression on the anterior surface of this is termed the pterygoid fovea.
The shape of the mandible depends largely upon the age of the individual, since it is determined to a great extent by the action of the muscles of mastication and by the presence or absence of teeth. Just as the alveolar portion developes with the eruption of the teeth and degenerates with their loss, so too the muscles of mastication modify the form of the mandible. In the new-born child the ramus joins the body at an oblique angle (see Fig. A111, which only later gradually becomes a right angle.
The mandible is the only bone of the skull that articulates with other skull bones in a moveable joint, the only bone (except the hyoid) that can be readily separated from the others, which are more or less firmly united by sutures.
The orbit is a paired cavity having the form of a four-sided pyramid placed horizontally; its apex is formed by the optic foramen and its base is surrounded by the margins of the orbit, the supraorbital and infraorbital. The four sides of the pyramid form the orbital walls, one of which is superior, one medial, one inferior and one lateral. Seven bones enter into the boundaries of the orbit, the frontal, sphenoid, ethmoid, lacrimal, maxilla, zygomatic and palatine.
The superior wall is horizontal and slightly concave. It is formed partly by the orbital portion of the frontal and to a lesser extent posteriorly by the lesser wing of the sphenoid.
The medial wall is almost sagittal an~ is mainly formed by the lamina papyracea of the ethmoid and, in front of this, by the lacrimal. The fronto-ethmoidal and fronto-lacrimal sutures form the boundary between this and the upper wall. In addition the maxilla takes part in the formation of the medial wall, firstly, by the orbital surface of its body below the lamina papyracea (see below) and, secondly, by its frontal process, which forms a narrow strip of the medial wall adjacent to the lacrimal bone.
The inferior wall passes without any boundary into the medial, but in the posterior two-thirds of the orbit and towards the lateral wall it is bounded laterally by the inferior orbital fissure. It is almost horizontal in position and is formed principally by the orbital surface of the maxilla and, to a small extent posteriorly, by the orbital process of the palatine.
The lateral wall is slightly concave and almost sagittal in position. It is more definitely bounded than the other walls in that in the whole of the hinder part of the orbit it is separated from adjacent walls by fissures. Between it and the upper wall is the superior orbital fissure and between it and the lower wall is the inferior orbital fissure. In its anterior part it is formed by the orbital surface of the zygomatic, in the posterior part by the orbital surface of the great wing of the sphenoid, the spheno-zygomatic suture separating these two surfaces.
The supraorbital margin is formed by the frontal bone, the infraorbital margin by the maxilla and zygomatic. The less sharply defined medial border is formed by the frontal process of the maxilla (anterior lacrimal crest) and the lateral border by the zygomatic.
The foramina and fissures in the orbit are:
In addition in the orbit, on the frontal bone, is the trochlear fossa (sometimes a spine) and the fossa for the lacrimal gland; in the region of the frontal process of the maxilla and the lacrimal bone, the fossa for the lacrimal sac, bounded by the anterior and posterior lacrimal crests; the infraorbital groove on the orbital surface of the maxilla; and the spine for the rectus lateralis on the great wing of the sphenoid.
The hard palate forms the roof of the mouth cavity. It is an elongated, semi-elliptical, strongly concave plate of bone, in whose formation the palatine processes of the maxillae and the horizontal portions of the palatines and partly also their pyramidal processes participate. It shows a median palatine suture, a transverse palatine suture and traces of an incisive suture. Anteriorly towards the front end of the median suture is the unpaired incisive foramen, by which the bony oral cavity communicates with both nasal cavities. Posteriorly in the horizontal portion of the palatine bone there is, on either side, the greater palatine foramen and in each pyramidal process the lesser palatine foramen. These paired foramina are the openings of the pterygo-palatine canal.
The bony nasal cavity is unpaired, but is divided into two symmetrical cavities by a median partition, the nasal septum, which is often oblique or not quite in the median line. Nine bones take part in the formation of the cavity; the nasal, frontal, ethmoid, sphenoid, maxilla, palatine, inferior concha, vomer and lacrimal. Its anterior opening is the piriform aperture, its posterior the choanae. The former is bounded by the nasal bones, the frontal processes and bodies of the maxilla; the choanae by the palatine bones, the medial plates of the pterygoid processes and the body of the sphenoid. The roof of the cavity is formed anteriorly by the two nasal bones and the nasal portions of the frontals, in the middle by the lamina cribrosa of the ethmoid and, posteriorly, by the body of the sphenoid. Its floor is the upper surface of the hard palate and is formed by the palatine processes of the maxillae and the horizontal portions of the palatine bones.
The nasal septum forms the medial wall for each nasal cavity and is itself formed by the lamina perpendicularis of the ethmoid anteriorly, and posteriorly and below by the vomer (see Fig. A82); the remaining portion is cartilaginous (see here).
The lateral wall of each cavity bears three nasal conchae. The lowest is a distinct bone, the inferior nasal concha, and is the largest and longest of the three, the uppermost being the smallest and shortest. The middle and upper conchae are projections of the ethmoid bone. By these three conchae the lateral portion of each cavity is divided into three passages (meatus); the superior meatus is between the superior and middle concha, the middle meatus between the middle and inferior and the inferior meatus between the inferior concha and the floor of the cavity. Above the superior concha, between it and the roof of the nasal cavity, there is a pocket-like depression, the spheno-ethmoidal recess. The part of the cavity medial to the conchae, between their medial edges and the septum, is termed the common meatus, the part behind the posterior ends of the concha the nasopharyngeal meatus. The following bones take part in the formation of the lateral wall; the ethmoid above and behind, the nasal surface of the frontal process of the maxilla above and in front, the body of the same bone below and in front, the perpendicular portion of the palatine behind and the medial surface of the lacrimal, which forms a small part in the anterior portion of the middle meatus. In addition to the principal nasal cavities there is a number of accessory cavities, which are air-containing, in most of the skull bones and especially those of the maxilla, the frontal, the sphenoid and the ethmoid (see here). The openings into the nasal cavities are also numerous and are:
The small pterygo-palatine fossa is situated between the anterior surface of the pterygoid process of the sphenoid, the perpendicular part of the palatine and the posterior end of the maxilla. It is funnel-shaped and passes below, without any demarcation, into the pterygoid canal, bounded by the same three bones. Above it opens into the inferior orbital fissure and laterally by the pterygo-maxillary fissure into the infratemporal fossa. Into it there are three openings; the foramen rotundum leading from the skull cavity, the opening of the horizontal pterygoid canal, which passes backward in the root of the pterygoid process to the foramen lacerum, and the spheno-palatine foramen leading into the nasal cavity.
The Hyoid Bone. The skull of the new-born child differs in many points from that of the adult. Instead of meeting in sutures the bones of the vault of the skull are connected by membrane, which in several places forms fontanelles (fonticuli). There are of these two unpaired and two paired. The frontal or great fontanelle (fonticulus frontalis) is rhomboidal in shape and lies at the meeting of the frontal, coronal and sagittal sutures, that is to say, between the two halves of the frontal bone, separated by a frontal suture, and the two parietals. The occipital or lesser fontanelle (fonticulus occipitalis) is triangular and lies at the hinder end of the sagittal suture, between the two parietal bones and the occipital. The sphenoidal fontanelles (fonticuli sphenoidales) are irregularly quadrangular and lie on each side between the sphenoidal angle of the parietal bone and the parietal angle of the great wing of the sphenoid, where later is the spheno-parietal suture. The mastoid fontanelles (fonticuli mastoidei) are, like the sphenoidal, of irregular shape and lie on either side between the mastoid angle of the parietal and the mastoid portion of the temporal, where later is the parieto-mastoid suture.
The squamous portion of the occipital shows a sutura mendosa, and the bone is represented by four distinct portions, the squamous, two lateral and basilar portions, separated by anterior and posterior intraoccipital synchondroses. In the temporal bone in place of the tympanic portion there is the anulus tympanicus (see here); the mastoid process is completely absent and the squamoso-mastoid suture separates the squamous portion from the pyramid, i.e. from the petrous portion and the mastoid. On the parietal the tuberosity is very distinct, as is also that of the frontal bone, which is still in two portions separated by the frontal suture. Between the sphenoid and the occipital there is a sphenooccipital synchondrosis and in the body of the sphenoid an intrasphenoidal synchondrosis.
The maxilla and mandible are low, the alveolar portions being quite wanting. The incisive suture is quite distinct on the hard palate. Between the two halves of the mandible the remains of a suture are visible; the rami are almost in the same line as the body, i. e. they form with it a very obtuse angle.
The hyoid bone is a small, flat bone situated at the base of the tongue. Although it has no direct connection with the skull and is situated in the neck below the mandible, it is usually described as a cranial bone. It presents a body (corpus), convex in front and concave behind, and two pairs of cornua. The greater cornua are long and thin and enlarged into a knob at their ends; they arise from the sides of the body and are directed upwards and backwards. The lesser cornua often remain cartilaginous, and are much smaller than the greater ones; they arise near the base of the greater ones and are directed posteriorly laterally and upwards.
The girdle of the upper extremity is formed of two bones, the scapula and the clavicle.
The scapula is a typical flat bone of triangular shape. Its anterior surface, turned toward the ribs, is termed the costal surface, its posterior surface, the dorsal surface. Its three angles are termed medial, inferior and lateral and its three borders, the superior, vertebral or medial and axillary or lateral.
The costal surface is smooth except for some transverse lines, lineae musculares, for the attachment of the subscapular muscle, and it is slightly concave, forming the subscapular fossa for the muscle of that name.
The dorsal surface is divided into two areas by a strong, roughened ridge the spine; the upper smaller area is the supraspinous fossa and the lower larger one the infraspinous fossa, which lodge muscles of the same names. The spine of the scapula is flat at the vertebral border, but becomes higher as it passes transversely across the dorsal surface, and at the neck of the bone it is prolonged into a flattened process, projecting over the lateral angle and termed the acromion. It presents a small surface for articulation with the clavicle (facies articularis).
The vertebral border is usually slightly and obtusely angled at the base of the spine; the axillary border is thick and rough for the attachment of muscles. The superior border presents a notch in the neighborhood of the lateral angle, the scapular notch, and between the notch and the lateral angle it gives rise to a strong hook-shaped coracoid process. This arises by a broad base and is at first directed upwards, but then bends forward and laterally.
The lateral angle bears the pear-shaped, slightly concave glenoid cavity for the reception of the head of the humerus. Both above and below it is a roughened area, the supraglenoid and infraglenoid tuberosities, which, give origin respectively to the tendons of the long heads of the biceps and triceps. The constriction of the scapula medial to the borders of the glenoid cavity is called the neck (collum) and in this region the supraspinous and infraspinous fossae become continuous. The medial angle is a right angle, the inferior one is more acute, but strongly rounded.
The clavicle is an S-shaped, long bone in which a middle portion, the body (corpus), and two extremities may be recognized; of the latter the medial is termed the sternal and the lateral the acromial extremity after the bones with which they articulate. The bone is convex anteriorly at its sternal extremity and concave anteriorly at its acromial extremity. The sternal end is thick and almost triangular-prismatic; the acromial end on the contrary is flattened.
At the sternal end there is a triangular sternal articular surface, which forms part of the sterno-clavicular articulation. Lateral from this on the anterior, lower border is a roughened area, the costal tuberosity, for the attachment of the costo-clavicular ligament. The body of the bone, like the sternal extremity, is almost triangular, but with strongly rounded angles.
The flattened acromial extremity at its boundary with the body and at its posterior and lower border bears a roughened area, the coracoid tuberosity, for the attachment of the coraco-clavicular ligament and, at its very end, an acromial articular surface for articulation with the acromion.
The humerus is a typical long bone, in which may be distinguished a long shaft or body (corpus) and two thickened extremities, superior and inferior. The superior extremity bears an articular head (caput), placed at an angle with the body and directed medially, It is almost hemispherical and is separated from the shaft of the bone by a shallow, circular groove, the anatomical neck (collum anatomicum). In addition to the head, the upper extremity bears two roughened elevations for muscular attachment; a larger one, the greater tubercle directed laterally, and a smaller one, the lesser tubercle, directed medially and anteriorly. Between the two is a distinct intertubercular groove. At the junction of the upper extremity with the body below the tubercles, there is a distinct diminution in the diameter of the bone, termed the surgical neck (collum chirurgicum).
The upper end of the shaft is almost cylindrical, but below the middle it becomes somewhat triangular and, at the same time, flattened. From each tubercle a ridge (crista) passes downwards, continuing the intertubercular groove for some distance. Below the greater tubercular crest there is a large, flat, roughened area; the deltoid tuberosity, for the attachment of the deltoid muscle; it is on the lateral, posterior part of the bone, which, at this level, is still cylindrical. At about the middle of the shaft on its medial surface there is a roughened area, not always distinct, for the attachment of the coraco-brachialis muscle and near this is a frequently large nutritive foramen.
From the middle of its length downwards the shaft of the humerus presents three surfaces, posterior, anterior medial, and anterior lateral. The two anterior surfaces are separated by a low elevation, but at the lateral angles there are sharp borders, medial and lateral. The lateral border begins below the deltoid tuberosity, being separated from it by a shallow groove, the groove for the radial nerve (musculo-spiral groove). This contains the radial (musculospiral) nerve and winds around the middle portion of the shaft in an open spiral, passing from above and medially, downwards and laterally and gradually flattening out. Its borders serve for the attachment of two heads of the triceps muscle. Towards the inferior extremity the humerus becomes markedly flattened and at the same time broader. The two borders are continued into two rough muscle projections, the medial border into the strongly projecting medial epicondyle and the sharper lateral border into the smaller lateral epicondyle. The former has on its posterior surface a shallow groove for the ulnar nerve, which is bounded laterally by the border of the trochlea.
Below the epicondyles is the lower articular head of the humerus, for the bones of the forearm. There is a separate surface for each of these, the large trochlea, hour-glass shaped, on the medial side for the ulna and the smaller, hemispherical capitulum laterally, for the radius. Above the trochlea on the medial anterior surface there is at the level of the epicondyle a rather deep depression, the coronoid fossa, and above the capitulum at the lower part of the lateral anterior surface there is a much smaller and shallower one for the head of the radius. Opposite these two fossae there is on the lower part of the posterior surface a broad and deep olecranal fossa.
The ulna is a distinctly triangular-prismatic long bone, thick above and much thinner below. It presents a superior extremity, a body or shaft (corpus) and an inferior extremity. The stout superior extremity carries the semilunar notch with the constricted, or even divided, articular surface for the trochlea of the humerus. Its anterior portion lies on the upper surface of the coronoid process, a broad, beak-like projection, while its posterior portion is on the anterior surface of a very strong, upwardly projecting process, the olecranon. On its lateral side the upper extremity has a notch lined with cartilage, the radial notch for the reception of the head of the radius. From it a rough ridge extends downwards on the upper part of the dorsal surface, the supinator crest, for the muscle Immediately below the coronoid process is a broad rough area, the ulnar tuberosity.
The shaft (corpus) of the bone is much thicker above than below, and at the same time becomes rounded below, the upper distinctly triangular portion becoming cylindrical in the lower fourth. An anterior or volar, a posterior or dorsal and a medial or ulnar surface may be recognized. The dorsal border separates the dorsal and medial surfaces and the volar border the volar and medial surfaces. The third border, turned toward the radius, is sharp; it separates the volar and dorsal surfaces and is termed the interosseous crest. The volar surface bears the nutrient foramen, otherwise the surfaces present no special markings.
The distal end of the bone, the inferior extremity, is the capitulum; it is rounded and covered by cartilage. On the radial side there is also an articular surface for the radius, the articular circumference, as well as a sharp process, projecting distally beyond the capitulum on the medial side, the styloid process.
The radius is the more lateral of the two bones of the forearm. In contrast to the ulna it is small above and broad and thick below.
The superior extremity is formed by the disk-shaped capitulum and a distinct circular constriction below this is termed the neck (collum). In its upper part the bone is almost cylindrical. The capitulum bears on its upper surface an articular depression or fovea for the capitulum of the humerus and a second articular surface, the articular circumference, that completely surrounds its margin. Below the neck on the upper part of the volar surface there is a distinctly elevated rough area, the tuberosity, which gives attachment to the biceps muscle.
The shaft (corpus) of the radius, like that of the ulna, is triangular-prismatic. The three surfaces are also placed as in that bone, so that a volar, a dorsal and a lateral (radial) surface may be distinguished and volar and dorsal borders as well as an interosseous crest. The last lies opposite the similarly named crest of the ulna and is the only sharp border of the radius, the others being rounded. The three surfaces present no markings of importance except some roughenings for muscles, such as that for the pronator teres. Usually a nutrient foramen occurs on the volar surface.
The inferior extremity is greatly broadened and flattened, so that in its region only a volar and a dorsal surface may be distinguished. The interosseous crest passes below into a slightly concave surface, the ulnar notch, which furnishes an articular surface for the capitulum of the ulna. Opposite it a styloid process projects beyond the general inferior surface of the bone; it is broader and less pointed than the similarly named process of the ulna.
The volar surface of the inferior extremity is smooth and slightly concave, the dorsal surface on the contrary presents distinct grooves with intervening ridges for the extensor muscles of the hand and fingers, one, especially deep and with an oblique course, being for the tendon of the extensor pollicis longus. On the distal terminal surface, which is turned toward the hand, there is a concave carpal articular surface, usually distinctly divided into two areas. By means of this surface the radius articulates with the navicular (scaphoid) and lunate bones of the hand.
The eight bones of the carpus are arranged in two rows, a proximal and a distal. Those of the proximal row, named from the radial side are the navicular (scaphoid), the lunate, the triquetrum or cuneiform, and the pisiform; those of the distal row named in the same order are the trapezium (greater multangular), the trapezoid (lesser multangular), the capitate or os magnum, and the hamate or unciform. The bones of the proximal row do not lie in a straight line, but form an arch, slightly convex proximally and deeply concave distally. Similarly from the row of distal bones, one, the capitate, projects strongly towards the bones of the proximal row and fills their concavity.
The carpal bones are very irregular in shape; they do not lie in a plane but form a dome, convex dorsally and concave volarly. The dome is increased by two bony projections on the radial and ulnar sides of the volar surface of the carpus, a deep groove, the carpal groove, lying between them. These projections are the ulnar and radial eminences. The latter is formed by the tubercle of the navicular (scaphoid) and the tubercle of the trapezium (greater multangular), the former by the pisiform and the hamulus of the hamate (unciform). The small, almost spherical pisiform bone lies on the volar surface of the carpus; all the other bones of the carpus have each a dorsal and a volar, more or less roughened surface. In the cases of the four bones at the sides of the carpus, the navicular (scaphoid), trapezium (greater multangular), triquetrum (cuneiform) and hamate (unciform), the dorsal and ventral surfaces are united by lateral ones, radial or ulnar. The numerous remaining surfaces are smooth, articular surfaces for articulation with the radius, the metacarpal bones or adjacent carpal bones. The pisiform has only one small, flat, articulating surface for articulation with the triquetrum (cuneiform); all the other bones have several. The more important of these surfaces are the following: The navicular (scaphoid) and lunate have each a convex surface for articulation with the distal end of the radius; the triquetrum (cuneiform) does not, however, articulate with the ulna, but with a triangular cartilage that separates it from the ulna. Between the proximal and distal rows, the joint between the convex head of the capitatum (os magnum) and the concavity formed by the lunate and navicular (scaphoid) is the most important. The first metacarpal articulates by a distinctly saddle-shaped surface with the trapezium (greater multangular), the second with the trapezoid (lesser multangulum), the third with the capitate (os magnum), while the hamatum (unciform) bears the two ulnar metacarpals.
The metacarpal bones are typical long bones, in which a proximal portion or base, a body (corpus) and a distal portion or capitulum may be distinguished. The bases articulate with the distal row of carpal bones, the capitula with the proximal row of phalanges. The metacarpal of the thumb is the shortest, that of the index the longest, and from this toward the little finger they gradually diminish in length.
The bases of the metacarpals are irregularly cubical; that of the thumb bears a saddle-shaped surface for articulation with the trapezium (greater multangular), the rest, in addition to the surfaces for the carpal bones, have also lateral surfaces for articulation with one another. The base of the third metacarpal bears a styloid process, which is directed laterally (radially).
The almost triangular prismatic bodies of the metacarpals, except that of the thumb, have each a volar and a dorsal angle; the latter broadens to a surface towards the capitulum, the former flattens towards the base. The capitula are spherical in shape; at their sides are depressions that give attachment to ligaments.
The bases are closely applied to one another, except in the case of the freely moveable metacarpal of the thumb; on the other hand, the bodies and the capitula are separated by considerable intervals, the interosseous spaces.
Each finger has three phalanges, the thumb only two. The basal phalanx is termed the first phalanx, the middle one the second phalanx and the distal or terminal one the third phalanx. The thumb lacks the second phalanx. The lengths of the phalanges diminish toward the finger tips, so that the basal phalanges are much the longest, terminal phalanges the shortest.
The longest phalanx is the basal one of the middle finger. The phalanges are long bones with a proximal extremity or base, a body (corpus) and a distal extremity or trochlea. The bases of the proximal phalanges have hollow spherical sockets for the capitula of the metacarpals, those of the middle and distal phalanges are hollow cylindrical, with a median elevation, corresponding in form to the trochleae.
The bodies of the phalanges are convex dorsally and flat or very slightly concave on the volar surfaces, with sharp lateral borders. The terminal phalanges have no trochleae, but the short bodies pass into a rough horse-shoe shaped enlargement, the unguicular tuberosity. At the distal ends of the proximal and middle phalanges there are foveae for the attachment of ligaments, similar to those on the metacarpal capitula.
In addition to the bones that have been mentioned there are in the hand a variable number of sesamoid bones. Two occur constantly at the metacarpo-phalangeal joint of the thumb and occasionally others are found at the corresponding joints of the index and little fingers and at the interphalangeal joint of the thumb. In the little finger they may be replaced by fibro-cartilage. In the thumb they are usually covered with cartilage on one side and are connected with the joint (see Fig. A224).
In the region of the metacarpus and fingers the bones of the hand do not form a flat surface, but a dome convex dorsally and concave volarly, which may be markedly deepened by the action of the muscles of the hand and also not a little flattened. The highest point of the convexity of the back of the hand is the metacarpal of the index finger. From this the curvature falls gradually toward the little finger and quite suddenly toward the thumb. The bones of the thumb, the metacarpal as well as the two phalanges, are placed with their surfaces directed laterally and medially, instead of dorsally and volarly as in the other fingers; the bones of the thumb, therefore; turn towards the dorsum of the hand a border and not a surface. In the metacarpal of' the little finger, also, the dorsal surface looks distinctly medially.
While the metacarpal bone of the index is the longest the phalanges of the middle finger are longer than those of the index, so that the middle finger is the longest of all the fingers. The phalanges of the ring finger are also usually longer than those of the index. Corresponding to the function of the hand as a grasping organ the fingers are strongly developed, forming almost half the length of the entire hand. The length of the carpus is about only 1/6 the length of the entire hand.
The innominate bone ( os coxae) consists until puberty of three bones united by synchondroses, the ilium, the pubis, and the ischium. All three bones meet in the articular cavity for the femur (acetabulum). The ilium forms the upper portion of the compound bone; it is the largest of the three bones and forms the upper third of the acetabulum. It consists of a body (corpus) and an ala. The pubis forms the lower and anterior portion of the innominate and the lower anterior third of the acetabulum. It is separated from the ischium by a large roundish foramen, the obturator foramen, but is also united with it in the inferior boundary of the foramen. It has a body (corpus) and two rami, a ramus superior, forming the upper boundary of the obturator foramen, and a ramus inferior. The ischium forms the lower posterior portion of the innominate, the lower posterior third of the acetabulum and the lower and posterior boundary of the obturator foramen. It consists of a body (corpus) and two rami, superior and inferior.
The ala of the ilium has somewhat the form of a broad flat shovel. At its central part it is often as thin as paper, but its upper border is thickened and rough and is termed the iliac crest. Upon this may be seen three parallel rough lines, most distinct at the middle of the crest, where it reaches its highest point. These lines are termed the outer lip, the inner lip and the intermediate lip. Anteriorly the crest ends in a projection, the anterior superior spine; at its posterior end is a less distinct posterior superior spine, and below this, separated from it by a slight notch, is the posterior inferior spine. Upon these there follows at the posterior end of the innominate a deep, parabolic notch, the great sciatic notch (incisura ischiadic a major); its upper boundary is the posterior border of the ala of the ilium. and its lower and anterior boundaries are the bodies of the ilium and ischium. Below the anterior superior spine, on the body of the ilium, is the anterior inferior spine.
The lateral surface of the ala is rough and convex and its principal markings are three rough lines, the posterior, anterior and inferior gluteal lines. The posterior line runs almost vertically over the posterior part of the ala to the upper boundary of the great sciatic notch. The longer anterior line runs from the anterior superior spine as an arch, at first almost horizontal and then almost vertical, to the upper border of the great sciatic notch where it ends not far from the posterior line. The inferior gluteal line is markedly shorter than the anterior, and forming a weak arch beginning between the anterior superior and anterior inferior spines, it runs above the acetabulum and almost horizontally to the middle of the great sciatic notch.
The medial surface of the ala of the ilium has two portions, a larger anterior one which is slightly convex and is termed the iliac fossa and an uneven posterior one. On the latter again there may be made out two portions, corresponding to portions of the sacrum with similar names, the lower and anterior auricular surface and the posterior and upper, very much roughened iliac tuberosity. The auricular surface is bounded by a slight paraglenoid groove. The iliac fossa is separated from the rest of the innominate by a line which is continued upon the pubis and is called the arcuate line; it forms a part of the boundary line (linea terminalis) separating the false and the true pelves. The body of the ilium forms the upper part of the acetabulum; it passes on the inner surface into the ala without demarcation and in the adult, in a similar manner, into the bodies of the pubis and ischium.
The pubis of the adult is intimately connected with the ilium and ischium and forms part of the acetabulum. Where the pubis and ilium meet there is a low, rounded elevation, the iliopectineal eminence. From the body of the bone there arises the triangular superior ramus, which lies almost horizontally and bears at its anterior end the elongated symphyseal surface for union with the bone of the opposite side; it also forms the upper boundary of the obturator foramen. On its upper surface is a sharp ridge, the pecten, which is a continuation of the arcuate line of the ilium. This ends anteriorly in a small elevation, the tubercle, not far from the symphyseal surface. Where the superior ramus arises from the body there is a broad obturator groove on the medial surface of the bone; it is bounded medially by the obturator crest. At the obturator groove anteriorly there is an elevation, the anterior obturator tubercle, directed toward the obturator foramen, and on the ischium a posterior tubercle. The inferior ramus passes obliquely downwards and laterally from the symphyseal surface.
The ischium forms the lower posterior part of the acetabulum, and in the adult passes over without demarcation into the ilium and pubis. It forms the lower anterior boundary of the great sciatic notch, below which it projects as a broad, flattened, but sharp spine. Below this is the lesser sciatic notch (incisura ischiadic a minor), which lies entirely in the ischium and whose lower boundary is a strong roughened protuberance, the tuberosity. From the neighborhood of this the inferior ramus ascends at a sharp angle to the superior ramus. With the lower ramus of the pubis it forms the lower boundary of the obturator foramen. The acetabulum is formed by the bodies of the three bones, but the lines of separation between these can be seen only in youthful bones. It is almost hemispherical, with elevated borders, and looks almost laterally. Below towards the obturator foramen there is a notch in its border, the acetabular notch. The bottom of the cavity shows two portions, the lunate surface, covered with cartilage, which forms the upper and lateral portions of the cavity, and the almost square, rough and uneven acetabular fossa, almost surrounded by the lunate surface.
In the femur there may be distinguished a superior extremity, a body or shaft (corpus) and an inferior extremity. The superior extremity bears the head (caput) at the extremity of a neck (collum), which passes into the shaft at an obtuse angle. The head is somewhat more than a hemisphere and is covered with cartilage, except at a slight depression near its center, the fovea. The neck (collum) is strongly constricted near the head but enlarges laterally toward the shaft of the bone; it has a long lower border and an upper border about half as long. At the upper end of the shaft, at the union of this with the neck are two large, strong processes, the trochanters. The greater trochanter is much larger than the lesser one and looks laterally. Its upper extremity, whose tip is slightly bent posteriorly and medially, projects above the neck and bears on the medial surface below the apex a trochanteric fossa. The great trochanter forms the entire lateral part of the upper extremity of the femur. The lesser trochanter is opposite the greater on the medial surface of the upper part of the femur and is a short conical projection directed medially and slightly backward; it lies at a somewhat lower level than the great trochanter. The two trochanters are connected on the anterior surface of the bone by a rough intertrochanteric line, and on the posterior surface by a distinct ridge, the intertrochanteric crest.
The shaft (corpus) of the femur is almost cylindrical, but toward its lower end it broadens and becomes triangular-prismatic with rounded borders. In this region there is an anterior medial, an anterior lateral and a posterior surface. It is distinctly convex anteriorly.
While the anterior and lateral surfaces of the bone are exceptionally smooth, the posterior surface shows a rough line, the linea aspera. This possesses two distinct lips, a medial and a lateral. Throughout the middle portion of the bone both lips lie close together, but above they diverge toward the two trochanters and below toward the epicondyles (see below). The lateral lip passes above into an elongated roughened ridge, the gluteal tuberosity, which is occasionally greatly enlarged to form the so-called third trochanter. The medial lip becomes less pronounced in its upper part and unites with the intertrochanteric line in the region of the lesser trochanter, without actually uniting with this latter, and so ends on the greater trochanter. Parallel with and somewhat lateral to it is a second rough line, the pectineal line, which passes upward toward the lesser trochanter.
Towards the lower end of the femur the two lips of the linea aspera gradually diverge from one another to bound a triangular, almost flat area on the posterior surface of the bone; this is the popliteal plane. Upon the linea aspera, above its middle, there is usually one or several nutrient foramina, that lead into canals directed distinctly proximally.
The inferior extremity of the femur is much broadened. It bears the two convex, backwardly directed articulating condyles, the larger medial condyle and the smaller lateral condyle, separated from one another behind by the intercondyloid fossa. The intercondyloid line separates the intercondyloid fossa from the popliteal plane. Anteriorly the cartilaginous surfaces of the condyles pass into a common articular surface, the patellar surface, which is concave transversely and convex sagittally; consequently, the whole cartilaginous surface at the lower end of the femur has a horse-shoe shape. Above the condyles are two rough, but only slightly prominent, processes, the medial and lateral epicondyles.
The patella is a flat disk-shaped bone, which is really a large sesamoid bone in the tendon of the Quadriceps femoris. Its upper border is broad and is termed the base, while below the bone passes into a point, the apex. The anterior surface is rough, the posterior smooth and in 2/3 of its extent covered with cartilage, this area taking part in the formation of the knee-joint and being called the articular surface. The posterior surface of the apex is, however, not covered with cartilage but is rough like the anterior surface.
The tibia is the medial and the larger of the two bones of the lower leg. It has a superior extremity, a shaft or body (corpus) and an inferior extremity.
The superior extremity is much the thickest portion of the bone. It bears medial and lateral condyles for articulation with the condyles of the femur. Their upper surfaces are the slightly concave medial and lateral superior articular surfaces which are separated by a median elevation, the inter condyloid eminence, surmounted by two tubercles, the medial and lateral intercondyloid tubercles. Both behind and in front of the eminence is a small shallow groove, the anterior and posterior intercondyloid fossae. Below the articular surfaces there is the rough, almost perpendicular border of the upper part of the bone, the infraglenoid border, and on the lateral and posterior part of this is an articular surface for the head of the fibula. Below the infraglenoid border on the anterior surface of the bone is a large roughened area, the tuberosity.
The shaft (corpus) of the tibia is distinctly triangular-prismatic. It is thick in its upper part, becomes gradually thinner lower down and then enlarges again below. It presents three surfaces and three borders. The medial and lateral surfaces are separated by the anterior crest, while the very sharp interosseous crest, directed toward the fibula, separates the lateral and posterior surfaces. The third, rounded border, the medial, separates the medial and posterior surfaces.
On the upper part of the posterior surface there is an oblique line, the popliteal line, which runs from the articular surface for the fibula downwards and medially to the medial border. Below this line is the nutrient foramen, usually large and distinct; it leads into a canal that runs obliquely downwards. The medial surface, like the anterior border, is subcutaneous and readily felt; the lateral surface shows no special markings. Towards the lower end the borders of the bone are rounded so that this part of the shaft is almost cylindrical.
The inferior extremity, which is thicker than the lower part of the shaft, is decidedly smaller than the superior extremity. It bears on its under surface a slightly concave inferior articular surface for articulation with the tarsus (talus). On its medial side there is a strongly projecting process, the medial malleolus, whose outer surface is also an articular surface for the tarsus and passes without demarcation into the inferior articular surface. On its posterior surface the medial malleolus has a broad medial malleolar groove for a muscle tendon. On its lateral surface the lower end of the tibia has a fibular notch for articulation with the lower end of the fibula; it is not, however, covered with cartilage.
The fibula is a long bone, very thin in proportion to its length; it is scarcely shorter than the tibia, beyond which it projects below. It lies on the lateral side of the lower leg and has a superior extremity, a shaft (corpus) and an inferior extremity. The superior extremity forms the head (capitulum) and the inferior extremity the lateral malleolus. The head is distinctly enlarged as compared with the slender shaft; its uppermost part is behind and somewhat lateral and is termed the apex. It bears, for articulation with the tibia, a small, almost flat surface, the capitular articular surface.
The shaft is very distinctly triangular-prismatic. The three surfaces are medial, lateral and posterior, the sharp borders, which are not always straight are termed crests. The anterior crest separates the medial and lateral surfaces, the posterior crest the posterior and medial surfaces and the lateral crest the posterior and lateral surfaces. In addition to these there is a feebly developed interosseous crest at about the middle of the medial surface, so that the fibula has really four borders.
The inferior extremity forms the lateral malleolus. This is longer and more pointed than the medial one and has upon its medial surface an articular surface, which immediately adjoins the inferior articular surface of the tibia. On the lateral surface of the malleolus there is a shallow groove for the peroneal tendons.
Like the hand, the foot consists of three portions:
but it differs from the hand not only in the number and form of its constituent bones, but also in certain special particulars. While the axis of the hand is the direct continuation of that of the forearm and arm, that of the foot is almost at right angles to that of the leg, and while in the hand the fingers are almost the half of its entire length, in the foot the tarsus forms almost the proximal half and the metatarsals and toes the distal half, the latter being only a fifth of the entire length of the foot.
The foot is more strongly arched than the bones of the hand and the arch is less capable of being modified. Its convexity is dorsal and the concavity plantar, the deepest point of the latter being at the sharp, lower edge of the second cuneiform bone. Similarly the dorsal surface of the second cuneiform is the highest point of the middle of the arch. The lower supports for the arch are the calcaneal tuberosity behind and the heads of the metatarsals in front. It is formed exclusively by the tarsus and metatarsus and is open medially, since the medial border of the foot is much higher than the lateral, which rests on the ground through almost its entire length.
The phalanges of the second to the fifth toes do not lie in a single plane, even when the toes are extended, but are strongly convex upwards and seem to be curved in a claw-like manner upon the heads of the metatarsal bones, so that only their distal ends are in contact with the ground. The second toe is the longest and is that through which the axis of the foot passes.
There are seven tarsal bones:
The arrangement of these bones is such that on the medial side of the foot there are three bones, the talus, navicular, and cuneiform, whereas on the lateral side there are only two, the calcaneus and cuboid. In contrast to the condition in the hand only a single bone, the talus, articulates with the lower leg bones.
The talus is a short bone with an irregular cubical form, and presents for examination a body (corpus), a head (caput), and a constricted portion between these, the neck (collum). The body is the thickest and most posterior part of the bone and bears on its upper surface an articular surface, the trochlea, covered with cartilage and articulating with the tibia and fibula. The trochlea extends also upon the lateral surface of the talus and upon a strong projection of the bone, the lateral process, forming the lateral malleolar surface; it extends also upon the medial surface forming the medial malleolar surface, but this is smaller in extent than the lateral one, a part of the medial surface being rough. Behind the trochlea is a backwardly projecting part of the bone, the posterior process, which bears a broad groove for the tendon of the Flexor hallucis longus. The under surface of the body bears a distinctly concave posterior calcaneal articular surface, in front of which is a broad depression, the sulcus tali. Anterior to this, in the region of the neck, there is on the under surface an elongated second articulation for the calcaneus, the middle calcaneal articular surface, and adjoining this, on the head of the talus, is an anterior calcaneal articular surface. The constricted neck (collum) is to be seen distinctly only on the upper and lateral surfaces; on the medial and lower surfaces it is clearly separated from neither the head nor body. The head (caput) is the rounded anterior end of the bone and bears the almost hemispherical navicular articular surface, for articulation with the navicular bone and navicular fibro-cartilage.
The calcaneus is the largest bone of the tarsus. Its principal part is termed the body (corpus), the posterior thickened end of which is termed the tuberosity (tuber calcanei) and projects backwards behind the other bones of the foot. On its under surface are two projections, the medial and lateral processes. Looking from above one sees three surfaces (posterior, middle, and anterior) for articulation with the talus; the posterior is the largest and is convex, the other two are slightly concave. Between the middle and posterior articular surfaces lies the calcaneal groove, which is broadly open laterally; with the sulcus tali it forms the sinus tarsi.
From the strongly concave medial surface of the calcaneus a broad process, the sustentaculum tali, projects towards the talus and bears the middle articular surface for that bone. On its under surface is the broad groove for the tendon of the Flexor hallucis longus, continuous with the similar groove on the talus. A similar, but much shallower, groove for the peroneal muscles lies on the lateral surface, which is otherwise flat, except that a small, blunt trochlear process sometimes occurs above the groove. The anterior surface bears the articular surface for the cuboid, which is somewhat saddle-shaped.
The navicular lies between the talus behind and the three cuneiforms in front. Its long axis is transverse to that of the foot and it is convex anteriorly and concave posteriorly; its dorsal surface is also distinctly convex. On its plantar surface, near the medial border, there is a strong rounded projection, the tuberosity.
The cuboid lies on the lateral border of the foot, between the anterior end of the calcaneus and the bases of the fourth and fifth metatarsals. It has an irregular cubical form, tapering toward the lateral border of the foot. Its anterior surface bears an articulating surface divided into two parts for the fourth and fifth metatarsals; its posterior surface is saddle-shaped and its medial surface has an articular facet for the external cuneiform. The plantar surface has a flat projection, the tuberosity, which is rounded and sometimes covered with cartilage; it serves as a pulley for the tendon of the Peroneus longus, which lies in a groove, the peroneal groove, in front of the tuberosity.
The cuneiform bones are wedge shaped; the internal one is the largest and has its sharp edge dorsally, while in the others it is turned plantarwards. The middle one is the smallest. They articulate with the navicular behind and the bases of three metatarsals in front; the internal one usually articulates also with the cuboid.
The metatarsals have each a base, a head (capitulum) and a body (corpus). They lie between the bones of the tarsus behind and the phalanges in front, articulating with both. In addition the bases of the second to the fifth articulate with each other. The first metatarsal is short and thick; the second is the longest. The base of the first has a broad tuberosity directed plantarwards and laterally, and a tuberosity also occurs on the base of the fifth which projects markedly upon the lateral border of the foot.
The phalanges resemble those of the hand but are markedly shorter. The great toe has two phalanges, which are much thicker than those of the other toes. Each phalanx has a base, a body, and a trochlea, this on the terminal phalanges being replaced by an unguicular tuberosity.
According to their outer form bones may be divided into three groups, long bones (ossa longa), short bones (ossa brevia) and flat bones (ossa plana). It is not, however, only on account of their external form that these three groups may be distinguished; they differ also in their structure, that is to say, in the arrangement of the two kinds of bone substance of which they are composed. These two kinds of bone substance are termed
To the long bones belong all the bones of the free extremities, with the exception of those of the carpus and tarsus and of the patella. Thus, the long bones are the humerus, ulna, radius, metacarpals, and the phalanges of the fingers; the femur, tibia, fibula, metatarsals, and the phalanges of the toes; the clavicle also belongs to this group. All these bones possess a marrow cavity. Notwithstanding their shape the ribs are not classified with the long bones since they do not possess a marrow cavity.
The short bones are the vertebrae, the bones of the carpus and tarsus, the patella, sesamoid bones and the hyoid.
The flat bones are the sternum, the scapula, the innominate bone ( os coxae), the ribs and most of the skull bones, including the mandible.
Certain bones of the human skeleton are not readily referable to any one of these groups, especially such bones as are formed by the fusion of several short bones or of short and flat bones. Such are known as irregular bones. Typical examples of these are the sacrum and the coccyx, both formed by the fusion of several short bones, and various skull bones, such as the temporal, the occipital and the sphenoid, which may be regarded as formed by the fusion of short and flat bones to a single skeletal structure.
The short bones have the simplest structure. They consist almost entirely of spongy substance, only a thin layer of a kind of compact bone, the so-called substantia corticalis, enclosing the spongiosa and forming the external boundary for the small marrow cavities (filled with red marrow) which occur between the bone trabeculae.
In the flat bones the part played by the spongy substance is markedly less and the more or less parallel bounding plates of compact bone are appreciably thicker. Indeed, where a flat bone is very thin the compact lamellae may be in contact, the spongy substance being entirely wanting. The fine spaces between the trabeculae of the spongy substance are occupied by usually red marrow. The flat bones of the skull present certain differences of structure. In place of a central spongiosa they have a much larger meshed, but still trabecular bone substance, the so-called diploë. This is enclosed between two relatively thick plates of compact bone, the outer one being usually thicker than the inner; these are termed the outer and inner vitreous tables. The wide spaces of the diploë contain blood-vessels, especially venous plexuses but no red marrow; where the bones become thin the diploë is greatly reduced and may even be wanting.
The greatest difference is seen in the structure of the long bones. The shaft (corpus) of these consists in almost its entire thickness of compact bone, which here reaches a greater development than in other bones. It forms a cylinder of compact substance and only towards the articulating ends does it enclose any considerable amount of spongy substance. These ends, however, are almost entirely formed of spongy substance, this being enclosed, as in the case of the short bones, only by an outer quite thin layer of compact cortical substance. At the junction of the articular extremities with the shaft, the small cavities between the trabeculae of the spongiosa, which contain red marrow, communicate with the cylindrical marrow cavity of the shaft; this contains yellow (in old age gelatinous) marrow.
The trabeculae and plates of the spongy substance, which are for the most part slender and thin, are not altogether irregular in their arrangement, but are influenced to a large extent both in their structure and their arrangement by pressure on the one hand and by the pull of muscles on the other. The spongiosa trabeculae strengthened in response to stress or strain are termed trajectories.
All figures are taken from the "Atlas typischer Röntgenbilder vom normalen Menschen" by R. Grashey (J. F. Lehmann, Munich).
While it is usual to study the bones of the human body in the macerated condition there is a method by which the parts of the skeleton may be made visible even in the living body, namely, the use of Röntgen rays. These readily penetrate all the soft parts of the body (all organic substance) and also cartilage, but cannot pass through the inorganic bone substance, and so by the use of Röntgen photography the bones alone are shown on the photographic plate. If the bones are not too far from the sensitized surface of the plate they appear relatively sharply outlined and undistorted, so that not only is their form made visible, but also the structure of the spongiosa is more or less evident. On the other hand, bones that are some distance from the sensitized surface of the plate appear distorted and with poorly defined outlines.
Consequently Röntgen pictures of the skull and of the pelvis are never anatomically satisfactory. But while a Röntgen picture of a bone is less satisfactory for study than the macerated bone itself, and while especially, the clearest Röntgen picture of the spongiosa is far inferior to what may be seen anatomically of the architecture of the substance in a macerated bone (Fig. A177, A178, A179, A180, A181), nevertheless the study of the bones in the living by means of the Röntgen rays is a material aid to their study by the direct, anatomical method. This is especially true in the case of young skeletons still developing; in these the Röntgen pictures are the more satisfactory since they show the ossification centres in their natural position in the transparent cartilage.
Table of Ossification (from Grashey)
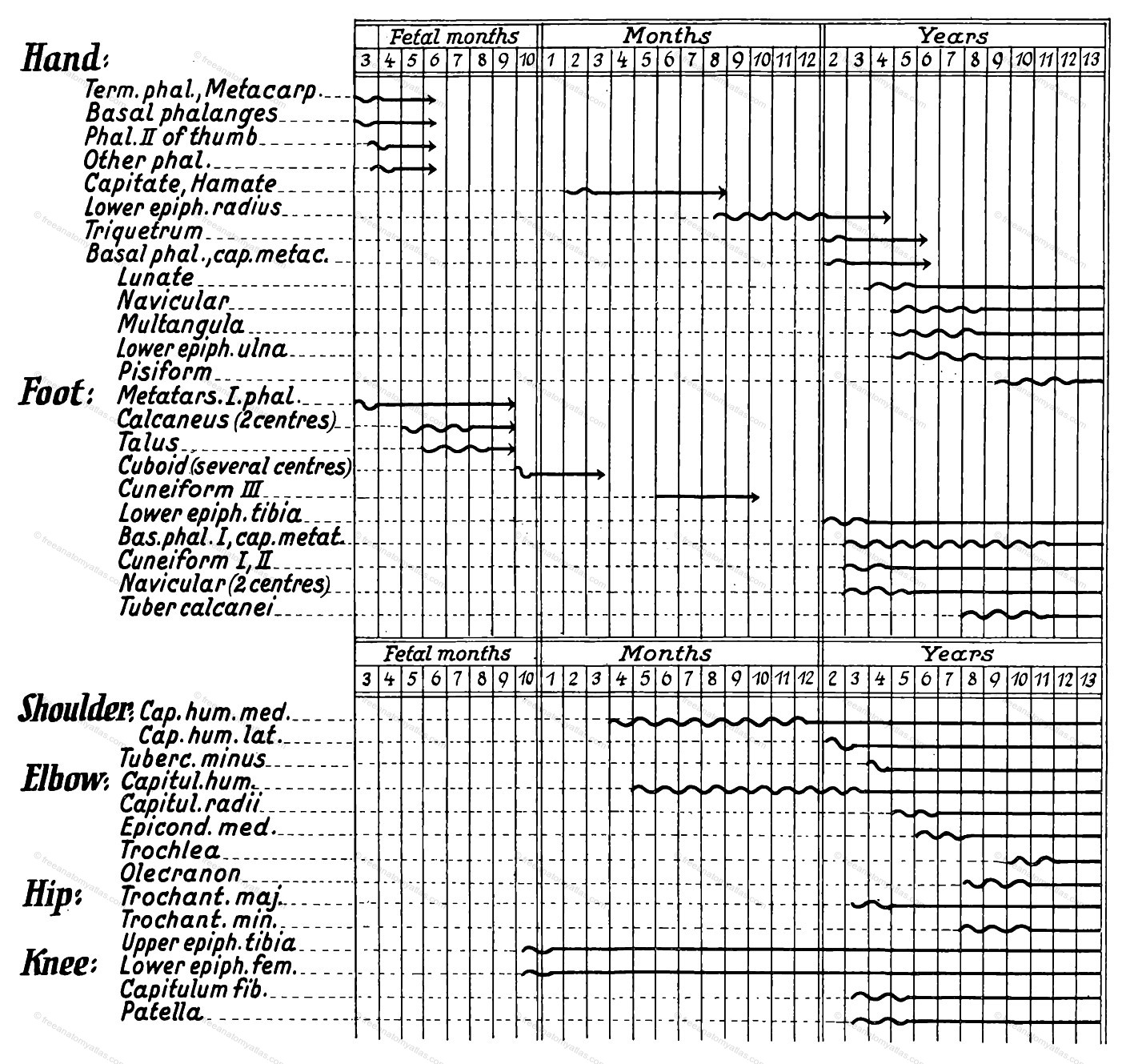
The wavy lines indicate the amount of variation in the appearance of the centres.
No portions of the skeleton are so well adapted for Röntgen photography as the bones of the hand, since the hand is flat and may be brought relatively close to the sensitized surface of the photographic plate; furthermore the bones have no great thickness and the defects (distortion and blurring) of Röntgen photography, sometimes so pronounced, are here hardly noticeable.
Consequently Fig. A187 not only shows the bones with almost perfectly sharp outlines, but the spongiosa and compacta of which they are formed are also evident. So too the marrow cavity of the long bones is shown. Since the figure is that of the hand of an individual of 28 years the development of the bones has been completed; the epiphyses of the long bones (see Figs. A184, A185, A186) have completely united with the diaphyses, whose ossification began in embryonic life.
The cavities of the joints always appear very broad in Röntgen photographs, since the articular cartilages do not show. The spaces between the bones in Röntgen photographs represent accordingly the articular cavities plus the articular cartilages of both bones concerned (compare Fig. A187 and A222).
Röntgen photographs also give exceedingly important information as to the ossification of the skeleton of the lower extremity. Of the epiphyses of long bones those that are the earliest to appear are those of the ends of the bones that enter into the formation of the knee-joint, the distal epiphysis of the femur and the proximal of the tibia, the former regularly and the latter frequently beginning to ossify before birth. That the ossification of the proximal end of the fibula begins much later is clearly shown in the accompanying figure, from which it may also be seen that the ossification processes not infrequently do not go on synchronously on the two sides of the body. Considerable variation also occurs in the time of the appearance of the ossification centres (see table here; ~~ = variation).
The ossification of the epiphyses proceeds in such a way that eventually there is a fusion with the diaphysial bone, the cartilaginous epiphysial disk that first separates them undergoing conversion into bone. On the other hand, on that surface of the epiphysis which forms the articular surface the ossification fails to invade the terminal layer of cartilage, which persists throughout life, forming the articular cartilage. According to the thickness of this cartilage, which varies to a considerable extent in the various joints, the articular cavity in Röntgen pictures will sometimes appear exceedingly wide and in other cases, narrow; Röntgen pictures can never give definite evidence as to the width of the articular cavity.
The bodies of the true vertebrae are united by fibrocartilaginous disks, the intervertebral fibrocartilages . Each of these consists of a firm ring, anulus fibrosus , of interlacing and concentric connective tissue bundles and of a central pulpy nucleus. The latter is compressed within the fibrous ring and bulges out when the disk is cut across. The fibrocartilages are in relation to the opposing surfaces of the bodies of adjacent vertebrae, these surfaces being covered by a thin layer of cartilage. The fibrocartilages are larger than the surfaces of the vertebrae between which they lie; their greatest height is at the middle, where they are in relation to the slightly concave surfaces of the vertebrae. There is no disk between the first and second vertebrae; the first lies between the second and third vertebrae and the last between the fifth lumbar vertebra and the sacrum, so that there are 23 fibrocartilages. In general they increase both in circumference and height from above downwards, just as do the vertebrae. In the cervical region they are, however, smaller but higher than those between the upper and middle thoracic vertebrae; those between the lumbar vertebrae are the largest and highest of all. The lowest fibrocartilages are wedge-shaped, being distinctly higher (about 1/3) in front than behind, especially in the case of the last one, the promontory.
In addition to the mixed synarthrotic union of the bodies, the true vertebrae are also connected by intervertebral articulations. Each pair of superior articular processes unite with the pair of inferior articular processes of the vertebra next above. Each joint has an articular capsule , loose in the cervical vertebrae but compact in the lower ones; it encloses the cartilaginous surfaces. There are no accessory ligaments.
Throughout the whole length of the vertebral column, in the region of the bodies, there is both an anterior and a posterior longitudinal ligament, covering respectively the anterior and posterior surfaces of the bodies and the intervertebral disks. The anterior one is a broad band, which begins quite small at the anterior tubercle of the atlas and broadens greatly below, where it ends on the anterior surface of the sacrum. It is very closely connected with the intervertebral fibrocartilages, but over the middle of the bodies, whose anterior surfaces are concave, it is more loosely attached. It consists of long superficial and deep fibers passing from vertebra to vertebra.
The posterior longitudinal ligament lies on the posterior surface of the bodies. It is much smaller than the anterior one and diminishes in breadth from above downwards. It begins as an independent ligament at the second vertebra, but is continued above this to the skull as the tectorial membrane (see here); below it ends in the sacral canal. It broadens distinctly over each intervertebral fibrocartilage and is closely connected with these, but has no attachments to the posterior surfaces of the bodies of the vertebrae.
The ligaments between the arches, ligamenta flava, are strong elastic bands, owing their name to their marked yellow color. They completely cover in the intervals between adjacent arches, extending anteriorly to the posterior borders of the capsules of the intervertebral articulations. Consequently they close in the vertebral canal up to the margins of the intervertebral foramina. Their inner surfaces are perfectly smooth and form a common surface with the inner surfaces of the arches. On account of their elasticity the posterior wall of the vertebral canal remains smooth during bendings of the column and they aid in the return of the vertebrae to the resting position. They begin between the second and third cervical vertebrae and extend to the last lumbar. They show a distinct groove in the middle line. Their number is 23 pairs.
The intertransverse ligaments, extending between the transverse processes of adjoining vertebrae, are unimportant. They are constant only in the thoracic region. The spinous processes of successive vertebrae are united by interspinous ligaments, which are most strongly developed in the lumbar region. They are united on one edge with the ligamenta flava and on the other. with the supraspinous ligament. This unites the tips of the various spinous processes and also runs over the tips as a continuous ligament. The interspinal and supraspinal ligaments occur through the entire extent of the true vertebrae and extend somewhat upon the sacrum also. For the sacral and coccygeal articulations see here.
The ribs unite posteriorly with the thoracic vertebrae in a joint; anteriorly they unite in a joint or a synchondrosis with the sternum or with one another. Only the last two ribs fail to unite with skeletal parts at their anterior ends. In the costo-vertebral articulations the head of a rib articulates with two adjoining vertebrae and the tubercle with a transverse process, except that this latter connection is wanting in the last two ribs, which articulate with only one vertebral body. The capitular articulations with the exception of the first and the two last, are characterized by the fact that the intervertebral fibro-cartilage between the two vertebrae which form the socket is attached to the head of the rib, forming the interarticular ligament and dividing the joint into two portions. The radiate ligaments, which radiate from the head of the rib upon the lateral surfaces of the articulating vertebrae, strengthen the weak articular capsules.
The costo-transverse articulations possess a loose capsule and are characterized by possessing a whole series of accessory ligaments. As a reinforcing band for the posterior surface of the capsule there is a quadrangular, short, tense tubercular ligament, which completely fills the space between the neck of the rib and the transverse process. The anterior and posterior costotransverse ligaments pass between the necks of the ribs and the transverse processes. The posterior are much weaker than the anterior and are attached to the articular processes of the vertebrae as well as to their transverse processes. The body of the vertebra together with the anterior ligament bounds a costo-transverse foramen, through which the anterior (intercostal) ramus of the spinal nerve makes its exit.
The cartilages of the true ribs unite with the sternum by the sternocostal articulations. The first cartilage, however, is always united to the manubrium by a synchondrosis. In the articulation of the second cartilage there is always a band passing to the end of the cartilage from the sternal synchondrosis; it is the interarticular ligament and it makes the joint two-chambered. In the sternal articulations of the third to the seventh rib the interarticular ligament is inconstant and frequently, when it is present, it divides the joint cavity unequally. Reinforcing the anterior surface of the joints are the radiate ligaments, which radiate out fan-like from the end of the cartilage upon the anterior surface of the sternum (see Fig. A212). Those of the lower ribs form by the interlacing of their fibres on the lower part of the sternum the sternal membrane. Between the cartilages of the seventh to the tenth ribs interchondral articulations may occur. Sometimes the sternal synchondrosis between the manubrium and the body of the sternum has a joint cavity.
For the movement of the head upon the vertebral column there is a combination of joints, including the atlanto-occipital articulations and the atlanto-axial (atlanto-epistrophic). Peculiar to the union of the first two cervical vertebrae with the occipital bone are the atlanto-occipital membranes, which serve to close the wide intervals between the atlas and the occipital and between the atlas and axis (epistropheus). The anterior membrane extends between the occipital and the anterior arch of the atlas, the posterior one, a continuation of the ligamenta flava, closes principally the gap between the occipital and the posterior arch of the atlas, but also extends between the posterior arch of the atlas and the arch of the axis (epistropheus).
The Atlanto-occipital articulations act as a symmetrical double joint. They are formed by the union of the occipital condyles with the superior articular surfaces of the atlas and according to the form of the articulating surfaces are ellipsoid joints. The articular capsule is rather broad and loose and lacks reinforcing ligaments.
The atlanto-axial (atlanto-epistrophic) articulation is formed by three separate joints;
The capsules of the atlanto-axial joint are wide and loose and are reinforced by a series of accessory ligaments. The very strong and firm transverse ligament arises from the medial borders of the lateral masses of the atlas and traverses its vertebral foramen, enclosing the dens from behind. It is cartilaginous where it passes over the dens and articulates with that process. From the middle of the ligament there is an upper and a lower prolongation. The upper one passes to the occipital bone, the lower inserts into the posterior surface of the body of the axis (epistropheus). The cruciform ligament so formed is termed the cruciate ligament. Three other ligaments belonging to the articulation are attached to the dens, a weak middle one and two strong lateral. The middle one, the apical ligament of the dens, is an unimportant thin band passing from the apex of the dens to the margin of the foramen magnum. The lateral ligaments, the alar ligaments, are much stronger and pass obliquely upward from the dens to the medial border of the occipital condyles, uniting the axis (epistropheus) directly with the skull. The ligaments of the joints are covered, towards the vertebral canal, by a broad firm sheet of fibres, the membrana tectoria, which is continuous with the dura mater at the foramen magnum and with the posterior longitudinal ligament below (see here).
The mandibular articulation is between the capitulum of the mandible and the mandibular fossa and articular tubercle of the temporal bone. The joint cavity is completely divided into two parts by an articular disk, whose circumference is united with the articular capsule. The capsule is rather loose and thin. It surrounds the mandibular fossa (except the non-cartilaginous portion), the articular tubercle and the head of the mandible, having its insertion on the neck. It is reinforced by a temporo-mandibular ligament, which passes from the zygomatic arch to the neck of the mandible.
Near the mandibular articulation, but without any direct connection with it, are the spheno-mandibular and stylo-mandibular ligaments. The former arises from the under surface of the great wing of the sphenoid near the angular spine and inserts into the lingua of the mandible. The latter arises from the styloid process and goes to the angle of the mandible. Both ligaments are weak and somewhat fascia-like, the stylomandibular spreading out directly into the fascia of the internal pterygoid muscle (bucco-pharyngeal fascia).
Besides these there are two other independent ligaments in the head. The pterygospinous ligament runs between the angular spine of the sphenoid and the upper end of the lateral plate of the pterygoid process. Sometimes it ossifies and then forms the pterygospinous process (Civinini). The stylo-hyoid ligament runs from the styloid process of the temporal to the lesser cornu of the hyoid. It frequently contains pieces of cartilage or bone, remains of the middle portion of the second branchial or hyoid arch from which the lesser cornu of the hyoid and the styloid process are formed.
Several clefts between the bones of the skull are also completely or partly closed by ligamentous masses as, for instance, the two orbital fissures, the spheno-petrous and petro-occipital fissures and the foramen lacerum, except where these give passage to nerves and vessels.
The sterno-clavicular articulation is between the clavicular notch on the manubrium of the sternum and the sternal articular surface of the clavicle. The two articular surfaces are made congruent by the interposition of an articular disk, which divides the joint cavity into two portions. The loose and thin articular capsule is strengthened over its entire surface by strong reinforcing ligaments. The sterno-clavicular ligament is fused with the anterior surface of the capsule and the interclavicular ligament unites the sternal ends of the two clavicles, extending across the jugular notch and resting on the upper border of the manubrium; it thus strengthens the upper surface of both sterno-clavicular joints. The costo-clavicular ligament is only functionally apart of the sterno-clavicular articulation. It is an independent, exceedingly strong ligament, passing between the cartilage of the first rib and the costal tubercle of the clavicle, and almost filling the interval between the sternal end of the clavicle and the first rib. Its rather short fibres are put on the stretch by a relatively slight abduction of the clavicle from the thorax.
The acromio-clavicular articulation is between the acromial articular surface of the clavicle and the articular surface of the acromion. Also in this joint there is a weak articular disk, which is frequently incomplete and may be entirely wanting. The articular capsule is strengthened over its upper, stronger portion by the acromio-clavicular ligament, which unites the ends of the adjoining bones. A very strong coraco-clavicular ligament unites the acromial end of the clavicle with the scapula, arising from the upper surface of the base of the coracoid process and passing to the coracoid tuberosity of the clavicle. It consists of two portions, an anterior flat, quadrangular trapezoid ligament and a posterior, triangular conoid ligament, small below and broad above (see Fig. A216).
On the scapula there are three independent ligaments:
The shoulder joint is between the glenoid cavity of the scapula and the head of the humerus. The glenoid cavity is relatively small arid only slightly concave, but it is materially enlarged and deepened by a strong, fibrous glenoidal lip, which surrounds the whole border of the bony socket. Nevertheless the socket of the joint is decidedly smaller than the articulating head, and free movement, accordingly, is not hindered by the socket, the joint being the most freely moveable joint in the body.
The articular capsule of the shoulder joint is wide and loose, as is necessary in a joint with free movement. Although it is on the whole thin, it receives strong reinforcements from the tendons of the muscles that pass over it (behind, the Supraspinatus, Infraspinatus, Teres minor; in front the Subscapularis) and from a strong reinforcing band, the coraco-humeral ligament. The articular capsule arises from the border of the glenoidal lip and inserts on the anatomical neck of the humerus. The coracohumeral ligament arises at the root of the coracoid process and is at first independent, but later becomes completely fused with the capsule and passes to an insertion in the neighborhood of the two tubercles on the anatomical neck of the humerus.
A peculiarity of the shoulder joint is that it is traversed throughout its entire length by a tendon, that of the long, head of the Biceps. The tendon arises at the supraglenoid tubercle, where it is fused with the upper part of the glenoidal lip, and runs through the cavity of the joint beneath the coraco-humeral ligament, and then along the intertubercular groove, being enclosed in this portion of its course by a prolongation of the capsule, the intertubercular sheath. The intertubercular groove is lined with cartilage throughout the extent of the sheath. Furthermore a thin-walled subscapular bursa, lying beneath the tendon of the subscapular muscle, also communicates with the joint cavity. This bursa is situated below the concave anterior surface of the coracoid process, between the coracohumeral ligament and a slight thickening of the medial surface of the capsule.
The elbow joint is a typical composite articulation, being composed, firstly, of the articulation of the trochlea of the humerus with the semilunar notch of the ulna, the humero-ulnar articulation; secondly, of that of the capitulum of the humerus with the capitular fovea of the radius, the humero-radial articulation; and, thirdly, of that of the radial notch of the ulna with the articular circumference of the radius, the proximal radio-ulnar articulation.
All three articulations are enclosed by a common articular capsule, which is broad and loose, especially anteriorly and posteriorly. It surrounds the olecranal, coronoid and radial fossae at the lower end of the humerus and is attached below to the ulna, close below the tip of the olecranon, to the border of the semilunar notch and to the tip of the coronoid process. The entire head of the radius and the greatest part of its neck is within the capsule. The radial collateral ligament extends from the lateral epicondyle of the humerus to the anular ligament, with which its fibres partly intermingle. The ulnar collateral ligament arises on the medial epicondyle of the humerus and passes, broadening as it goes, to the border of the semilunar notch of the ulna. The anular ligament is a dense firm band that surrounds the head of the radius like a sling. It arises from the anterior border of the semilunar notch of the ulna and is inserted into the posterior border of the radial notch of the same bone, forming with the latter notch the socket of the proximal radio-ulnar joint, 3/4 of this socket being formed by the ligament and 1/4 by the notch. On its inner surface, which is turned toward the cartilage-covered articular circumference of the head of the radius, the ligament is perfectly smooth. Below it the capsule is thin and projects slightly at the neck of the radius to form the sacciform recess.
Functionally considered the elbow joint is a combination of only two joints, since the humero-radial articulation does not act as an independent mechanism. There is, then, in the first place, the humero-ulnar articulation, which is a hinge joint, and, secondly, the proximal radio-ulnar articulation, which is a pivot joint.
The obtuse angle, open radially, formed by the upper and lower arm bones when the limb is extended, is termed the arm angle.
The radius and ulna are connected throughout almost their entire length by the interosseous membrane, which is attached to the interosseous crests of the two bones, except above, where the interosseous space persists. In addition the two bones are united by the the chorda obliqua, which passes from the coronoid process of the ulna to the lower border of the tuberosity of the radius.
The distal radio-ulnar articulation is between the articular circumference of the head of the ulna and the ulnar notch of the radius and also the articular disk which separates the head of the ulna from the cuneiform (triquetral) bone, the socket for the head of the ulna being formed partly by the ulnar notch and partly by the articular disk. Part of the socket is, therefore, nearly in the vertical plane and part almost horizontal, so that the head of the ulna rests upon the lateral as well as the lower surface of the socket. The capsule sends a sacciform recess upwards between the two bones of the forearm. The articular disk is attached on the one hand to the ulnar border of the lower part of the radius, where it is continuous with the articular cartilage, and on the other hand to the styloid process of the ulna.
The joints of the hand are those of the carpus and those of the fingers. The carpal joints are:
The finger joints are the metacarpo-phalangeal and the inter-phalangeal.
The radio-carpal articulation is between the carpal articular surface of the radius, together with the articular disk, and the proximal surfaces of the first row of carpal bones, the navicular and lunate articulating with the radius and the triquetrum (cuneiform) with the disk. The joint is completely separated from the intercarpal joint by short ligaments extending between the three bones, the navicular (scaphoid), lunate and cuneiform (triquetrum). The articular capsule is lax and thin and encloses the cartilaginous articulating surfaces.
The intercarpal articulation is between the first and second rows of carpal bones, the first row forming essentially the socket for the head of the capitate (os magnum) and the proximal part of the hamate (unciform). The line of the joint is S-shaped and its cavity usually communicates between the capitate (os magnum) and lesser multangular (trapezoid) with the carpo-metacarpal joint. The articular capsule is thin.
The articulation of the pisiform bone is between the pisiform and cuneiform (triquetral) bones. The piso-uncinate (piso-hamate) and the piso-metacarpal ligaments, passing respectively from the pisiform to the hamulus of the unciform (hamate) and to the base of the fifth metacarpal, are merely continuations of the tendon of the flexor carp ulnaris.
The common carpo-metacarpal articulation is between the bases of the second to the fifth metacarpals and the distal articular surfaces of the lesser multangular(trapezoid), capitate (os magnum) and hamate (unciform). The joint cavity usually communicates with that of the intercarpal joint and sometimes is divided transversely into two parts. The articular capsule is tense and firm. The joint cavity extends a short distance between the bases of the metacarpals.
The carpo-metacarpal articulation of the thumb is always independent, neither communicating with the other carpo-metacarpal joints nor with the intercarpal. The articulating surfaces are saddle-shaped, more markedly so than in any other joint in the body.
Only one of the carpal ligaments arises from the ulna, the ulnar collateral ligament, which arises from the styloid process of that bone and is attached to the triquetrum (cuneiform). Corresponding to it on the radial side is the radial collateral ligament, passing from the styloid process of the radius to the navicular (scaphoid). In addition, the dorsal radio-carpal ligament extends obliquely from the dorsal surface of the lower end of the radius to the dorsal surfaces of the bones of the first row of the carpus, and the corresponding volar radio-carpal ligament passes, not only to the bones of the first row, but also to the capitate (os magnum). In the depth of the carpal groove, ligaments converge to the capitate (os magnum) forming the radiate ligament. The remaining carpal ligaments, which unite the carpal bones either with each other or with the metacarpals are the volar and dorsal intercarpal, the volar and dorsal carpo-metacarpal and three volar and four dorsal interosseous ligaments, these last filling the intervals between the bases of the metacarpals.
The metacarpo-phalangeal articulations are between the heads of the metacarpals and the bases of the proximal phalanges. Collateral ligaments strengthen their sides and accessory volar ligaments their volar surfaces, while the transverse capitular ligaments unite the heads of the four ulnar metacarpals. The articular capsules of the interphalangeal articulations are strengthened laterally by collateral ligaments. Imbedded in the metacarpo-phalangeal joint of the thumb there are two sesamoid bones, and smaller and inconstant ones may be found in the corresponding joint of the index and little fingers.
The apex of the sacrum and the first coccygeal vertebra are united by the sacrococcygeal symphysis and also by a number of rather unimportant ligaments. On the anterior surface is the anterior sacro-coccygeal, at the sides the lateral sacro-coccygeal and behind the posterior sacro-coccygeal ligaments, The last have a superficial portion, which unites the sacral and coccygeal cornua, and a deep portion, which is the lower end of the posterior longitudinal ligament (see here).
The symphysis pubis is an amphiarthrosis uniting the symphyseal surfaces of the two pubic bones. The union is by an interpubic fibrocartilage, which frequently contains a slit-like cavity. Strengthening the symphysis there is a superior pubic ligament, which stretches from one pubic tubercle to the other over the upper border of the symphysis, and an arcuate ligament at the lower border.
The posterior joint of the pelvic girdle, the sacro-iliac articulation, is paired and is formed by the auricular surfaces of the sacrum and ilium. It is an almost immoveable joint, since the irregular curved and uneven surfaces do not lend themselves to any extensive movement. The contact of the two bones is further maintained by a strong ligament, the interosseous ligament, which unites the tuberosities of the bones, so that these are united anteriorly by a joint, posteriorly by a syndesmosis.
In addition to the interosseous ligament there is also a posterior sacro-iliac ligament, which consists of a superficial long and a deep short sacro-iliac ligament and is formed by a number 'of oblique fibre bundles that pass from the posterior part of the tuberosity of the sacrum to the crest of the ilium in the neighborhood of the posterior superior spine. A weaker anterior sacro-iliac ligament is merely a thickening of the anterior surface of the articular capsule.
Finally the ilio-lumbar ligament unites the ilium to the fifth lumbar vertebra. It is a strong band which passes from the transverse process of the fifth (sometimes also the fourth) lumbar vertebra to the crest of the ilium. By it the last lumber vertebra and the last intervertebral fibrocartilage become part of the boundary of the pelvis.
The obturator membrane closes the obturator foramen, except for a small area at the upper part of the foramen where the obturator groove begins.
The sacro-tuberous (great sacro-sciatic) ligament arises from the lateral portions of the posterior surfaces of both the sacrum and coccyx, from the posterior part of the crest of the ilium and its posterior superior and inferior spines. It concentrates to a broad firm band which is attached to the ischial tuberosity. A prolongation of it along the lower borders of the inferior rami of the ischium and pubis is termed the falciform process.
The much shorter sacro-spinous (lesser sacro-sciatic) ligament lies on the pelvic side of the sacro-tuberous and arises from the lateral border of the lower part of the sacrum and of the upper part of the coccyx; it is inserted into the spine of the ischium. It converts the great sacro-sciatic notch into a roundish, quadrangular foramen, the great Sacro-sciatic foramen. With the sacro-tuberous ligament it converts the lesser sacro-sciatic notch into the lesser sacro-sciatic foramen. The sacro-spinous ligament separates these two foramina and forms part of the pelvic outlet.
The pelvis is bounded by the following bones, the innominates (coxae), the sacrum, the coccyx, and the fifth lumbar vertebra. In addition certain ligaments or membranes take part in its boundaries, the interpubic fibrocartilage, the obturator membrane and the sacro-spinous, sacro-tuberous and ilio-lumbar ligaments.
There may be distinguished a great or false pelvis (pelvis major) and a small or true pelvis (pelvis minor). The former is much more capacious than the latter and it is only partly bounded by bones, the ala of the ilia and the fifth lumbar vertebra. Its separation from the true pelvis is indicated by the linea terminalis.
The true pelvis is a short canal with for the most part bony walls, the front wall being quite short, while the posterior one is markedly longer.
The inlet of the true pelvis (apertura superior) is bounded by the promontory, the three parts, sacral, iliac (linea arcuata) and pubic (pecten), of the terminal line and the upper border of the interpubic fibrocartilage or rather the superior pubic ligament.
The boundaries of the pelvic cavity are, behind, the concave pelvic surface of the sacrum and the anterior surface of the coccyx; laterally the pelvic surfaces of the bodies of the ilium, ischium and pubis, the sacro-tuberous and sacro-spinous ligaments, the rami of the pubis and ischium and the obturator membranes; anteriorly, the symphysis pubis and the anterior ends of the pubic bones. The anterior wall is by far the shortest, the posterior the longest. Posteriorly on the lateral walls are the two sacrosciatic foramina, the upper and larger one being rounded quadrangular, and the lower smaller one triangular.
The outlet (apertura inferior) is bounded by the arcuate ligament, the symphysis, the ischial tuberosities, the inferior rami of the pubes and ischia, the sacro-tuberous ligaments and the apex and lateral borders of the coccyx. In contrast to the inlet the boundary of the outlet is not in one plane. Its deepest point is formed by the coccyx and the ischial tuberosities also project strongly downwards, while in the region of the sacro-tuberous ligament and symphysis pubis the boundary slopes to a higher level. The angle that the two lower pubic rami form with the symphysis is termed the pubic angle and is somewhat rounded off to a pubic arch by the arcuate ligament.
The pelvis is not placed horizontally in the body but is inclined. Its inclination varies, being on the average about 60°(inclination of the plane of the inlet to the vertical). The pelvis, and especially the true pelvis, more than any other part of the skeleton shows sexual differences. In the female the false pelvis is lower, broader and flatter, and the ala of the ilium are usually less strongly concave. The cavity of the true pelvis is larger. Its inlet in the male is heart-shaped on account of the greater projection of the promontory; in the female it is transversely oval. The outlet in the male is more strongly narrowed than in the female, owing to the ischial tuberosities being somewhat convergent. The pubic angle in the male is acute, about 75-80°; in the female it is a right angle or obtuse, 90-100°. For the inguinal ligament see here.
The Inguinal ligament (Poupart's) arises from the anterior superior spine of the ilium and passes, tensely stretched, to the pubic tubercle, where it has a broadened insertion. An almost horizontal reflexion of the ligament extends from the insertion to the upper border of the superior ramus of the pubis, forming the lacunar ligament (Gimbernat's). The inguinal ligament is the tendinous lower edge of the aponeuroses and fasciae of the abdominal muscles, and does not properly belong to the ligaments of the pelvis.
The hip joint (articulatio coxae) is between the acetabulum of the innominate bone and the head of the femur. The socket is materially deepened by a strong, fibrocartilaginous glenoidal lip, triangular in cross section, so that it embraces more than half the spherical head. Consequently the joint is a typical ball and socket arrangement (enarthrosis). The glenoidal lip bridges the acetabular notch, converting it into a wide foramen; in this part of its extent the lip is termed the transverse ligament.
The articular capsule is greatly strengthened by reinforcing bands and is the strongest in the body. It takes origin around the base of the glenoidal lip and encloses not only the head of the femur but also the greater part of its neck. Anteriorly it is attached to the intertrochanteric line, but posteriorly it does not extend so far down, enclosing on that surface only a little more than half the neck. On account of the thickness of the capsule the extent of the joint cavity is somewhat less.
The reinforcing ligaments of the capsule are firmly united with it and may be either longitudinal or circular. The latter, forming the orbicular zone, surround the neck of the femur at its narrowest part and have a circular course in the inner layers of the capsule, firmly united to the longitudinal fibre bundles. A longitudinal ligament arises from each of the constituent parts of the innominate bone and they are thus three in number, the ilio-femoral, the pubo-capsular and the ischio-capsular.
Much the strongest of the three ligaments is the thick ilio-femoral ligament, one of the thickest ligaments of the body. It arises from the body of the ilium in the region of the anterior inferior spine and passes obliquely on the anterior surface of the capsule to the intertrochanteric line, which is produced by the ligament. The pubo-capsular ligament arises from the upper ramus of the pubis and passes on the medial surface of the capsule toward the lesser trochanter. The ischio-capsular ligament arises from the body of the ischium and passes on the posterior wall of the capsule for the most part to the orbicular zone, but in part also beyond this towards the lesser trochanter.
It is a peculiarity of the hip joint that its socket is not lined with cartilage over the area of the acetabular fossa, this being occupied by a pad of fat. From it as well as from the acetabular notch a characteristic ligament arises, the ligamentum teres, which is a flat, but sometimes strong, band, containing blood vessels, that is inserted into the fovea on the head of the femur. In the complete joint it lies upon the fat pad of the acetabular fossa and on account of its length and weakness does not limit materially the movements in the joint.
The thinnest parts of the capsule are situated on its lower wall, between the pubocapsular and ischio-capsular ligaments and above the orbicular zone, between the ischiocapsular and ilio-femoral ligaments. The anterior wall is also thin between the ilio-femoral and pubo-capsular ligaments, where occasionally a communication occurs between the joint cavity and the ilio-pectineal bursa, situated beneath the ilio-psoas muscle.
The knee joint (articulatio genus) is between the condyles and patellar surface of the femur on the one hand and the condyles of the tibia on the other. In addition, the articular surface on the posterior surface of the patella takes a passive part in the formation of the joint.
On account of its form and the multiplicity of its parts the knee joint is one of the most complicated joints of the body. The line of attachment of the articular capsule follows in general the margins of the cartilage-covered surfaces; on the posterior surface of the femur the intercondyloid line indicates the line of attachment, so that the whole intercondyloid fossa is excluded from the joint cavity.
The tibial collateral ligament is connected with the capsule. It arises from the medial epicondyle of the femur and passes, always intimately connected with the capsule, by its superficial fibers to the medial border of the tuberosity of the tibia and by short deep fibres, directed obliquely backwards, to the medial meniscus and the infraglenoid margin of the medial condyle of the tibia. The fibular collateral ligament, on the contrary, is for the most part separated from the capsule by fat tissue and consequently appears as an independent firm, rather flat and relatively small ligament, extending between the lateral epicondyle of the femur and the head of the fibula.
On the posterior wall of the capsule there are two reinforcing ligaments. The oblique popliteal ligament is a prolongation of the tendon of the semi-membranous muscle and runs obliquely from below and medial, upwards and laterally over the posterior surface of the capsule, in which it loses itself. The arcuate popliteal ligament is an arched band which curves over the tendon of origin of the popliteus muscle and also radiates out in the capsule. Some of its fibres pass to the head of the fibula and form what is termed the retinaculum of the arcuate ligament.
The anterior wall of the knee joint is formed almost entirely by the tendon of the quadriceps muscle and the patella. The quadriceps tendon is actually attached to the base of the patella, but it is continued by the flat, very strong patellar ligament, which passes from the apex of the patella to the tuberosity of the tibia. It is independent of the knee joint and unconnected with its capsule. A constant deep infrapatellar bursa, separates the ligament from the anterior surface of the upper part of the tibia. Tendinous prolongations from the quadriceps tendon, the medial and lateral patellar retinacula, strengthen the anterior part of the articular capsule.
The synovial folds of the knee joint are the alar and patellar folds. The former are formed largely of fatty tissue and lie behind the patellar ligament, where masses of fat covered by the synovial membrane of the joint bulge into the joint cavity forming medial and lateral alar folds. The patellar fold (ligamentum mucosum) is a fibrous and usually fat-containing band of variable thickness, that arises, between the alar folds and connected with them, from the front wall of the capsule and is attached behind in the intercondyloid fossa.
Of the outpouchings of the joint cavity the largest is the suprapatellar bursa, which extends for almost a hand's breadth beneath the tendon of the quadriceps. It is in wide communication with the joint cavity and into its upper wall the fibers of the quadriceps that form the articularis genus muscle are inserted. The posterior wall of the bursa does not rest directly on the femur, but on an interposed fat pad. Two or three much smaller outpouchings of the capsule occur on its posterior wall, the popliteal bursa under the tendon of the popliteus, the semimembranosus bursa under the tendon of the semimembranosus, and the medial gastrocnemial bursa under the tendon of the medial head of the gastrocnemius. The last two may unite. (See Figs. A323 and A324.)
Two discoidal or semilunar fibrocartilages rest on the condyles of the tibia, the medial and lateral menisci. They are not attached to the condyles, but to the capsule by their outer margins and to the intercondyloid eminence and the cruciate ligaments. In section they are wedge shaped. The medial meniscus is smaller than the lateral and almost semicircular; it forms, however, an arc of a greater circle than does the lateral, which is almost circular and open only at its attachment to the intercondyloid eminence. It is broader than the medial and, since its radius is smaller, it covers the condyle of the tibia except over a relatively small central area. The lateral meniscus is attached to the anterior intercondyloid fossa and to the lateral intercondyloid tubercle, the medial one extends from the anterior border of the medial condyle of the tibia to the posterior inter-condyloid fossa. The two menisci are connected anteriorly by a very variable transverse ligament.
In addition to the menisci there are associated with the knee joint two remarkably strong ligaments, the cruciate ligaments. They arise from the intercondyloid fossa of the femur and pass to the intercondyloid tubercles or fossae of the tibia. The anterior cruciate ligament passes between the medial surface of the lateral condyle of the femur and the anterior intercondyloid tubercle and fossa of the tibia, and the posterior cruciate ligament arises from the lateral surface of the medial condyle of the femur and passes to the posterior intercondyloid tubercle and fossa of the tibia. The two ligaments, of which the posterior is usually the stronger, cross one another in passing from one bone to the other. The posterior one is usually connected with the lateral meniscus.
The tibio-fibular articulation is between the fibular articular surface of the femur and the articular surface on the head of the fibula. It is a pronounced amphiarthrosis, with almost flat articular surfaces and with strong connecting bands on its anterior and posterior surfaces, the fibular capitular ligaments. Rarely the joint communicates with the knee joint through the popliteal bursa.
The interosseous membrane is very similar to that of the forearm and like this, extends between the interosseous crests of the two bones. In its upper part it has a large perforation for the passage of vessels.
The tibio-fibular syndesmosis is formed by two ligaments, rich in elastic fibres, extending on the anterior and posterior surfaces between the lower ends of the tibia and fibula. They are the lateral malleolar ligaments and are put on the stretch when the broader anterior part of the talus is brought between the two bones, the stretching being possible on account of the elastic fibres of which the ligament is largely composed.
The ankle joint (talo-crural articulation) is between the talus and the two bones of the lower leg. The articular surfaces are the trochlea of the talus on the one hand and on the other hand the inferior surface of the tibia, the articular surface of the medial malleolus and that of the lateral malleolus. The thin articular capsule surrounds the articular surfaces.
The group of ligaments that radiate from the medial malleolus to the talus, calcaneus and navicular constitutes what is termed the deltoid ligament. It consists of four not very distinctly separate ligaments, the anterior and posterior talo-tibial, the calcaneo-tibial and the tibio-navicular. The first of these passes to the anterior part of the neck of the talus and is completely covered in by the calcaneo-tibial. This is attached to the border of the sustentaculum tali, while the posterior talo-tibial goes to the posterior process of the talus and the tibio-navicular to the dorsal surface of the navicular.
Three distinctly separate ligaments pass from the lateral malleolus to the talus and calcaneus, the anterior and posterior talo-tibular and the calcaneo-tibular. The first of these runs almost horizontally from the anterior surface of the malleolus to the anterior border of the trochlea of the talus; the second, also horizontal, passes to the lateral tubercle of the posterior process of the talus; and the calcaneo-fibular passes obliquely downward and backward to the lateral surface of the calcaneus.
The talo-calcaneal articulation is between the posterior articular surface of the calcaneus and the posterior calcaneal facet of the talus. The latter is concave, the former convex. Occasionally the joint cavity communicates with that of the ankle joint.
The talo-calcaneo-navicular articulation is between the head of the talus on the one hand and the anterior and middle articular surfaces of the calcaneus, the posterior surface of the navicular and the navicular fibrocartilage in the plantar calcaneo-navicular ligament (see here). The socket for the head of the talus is thus formed by four different cartilage-covered surfaces. It is a composite joint, being a combination of the anterior and middle talo-calcaneal and the talo-navicular articulations.
The ligamentous connections of the talus and calcaneus are, firstly, the interosseous talo-calcaneal ligaments which fill the sinus tarsi and, secondly, reinforcing ligaments of the posterior talo-calcaneal joint, the medial, lateral, posterior and anterior talo-calcaneal ligaments. The lateral and anterior ligaments, which bridge over the sinus tarsi, are united with the interosseous ligament, the posterior one extends between the lateral tubercle of the posterior process of the talus and the upper surface of the calcaneus, and the medial passes from the tubercle of the talus to the sustentaculum tali.
The calcaneo-cuboid articulation is between the cuboid surface of the calcaneus and the posterior surface of the cuboid. The surfaces are almost saddle-shaped. With the talo-navicular articulation it formes the transverse tarsal articulation (Chopart's).
The cuneo-navicular articulation is between the anterior surface of the navicular and the posterior surfaces of the three cuneiform bones and extends between the cuneiform bones themselves, and between the lateral surface of the cuboid and the corresponding surfaces of the navicular and lateral cuneiform. As a rule the joint also communicates between the medial and middle cuneiforms with the second tarso-metatarsal articulation.
The tarso-metatarsal articulations (Lisfranc's articulation), together with the intermetatarsal articulations, are three joints, one between the metatarsal of the great toe and the medial cuneiform, a second, between the bases of the second and third metatarsals and the middle and lateral cuneiforms, and a third, between the fourth and fifth metatarsals and the cuboid. The line of the joints is a curve convex anteriorly with a deep backward indentation between the middle cuneiform (short) and the base of the second metatarsal (long).
The dorsal tarsal ligaments pass from the talus and calcaneus on the one hand to the navicular and cuboid on the other. They are the dorsal talo-navicular, the dorsal calcaneo-navicular and the bifurcated ligaments. The latter unites the anterior medial angle of the calcaneus with the dorsal surfaces of the navicular and cuboid, dividing into two parts corresponding to the two bones.
The dorsal naviculari-cuneiform ligaments unite the navicular bone with the cuneiforms; the dorsal cuboideo-navicular, the cuboid with the navicular; the dorsal intercuneiform, the three cuneiforms with one another; and the dorsal cuneo-cuboid, the lateral cuneiform and the cuboid. The dorsal tarso-metatarsal ligaments unite the bases of the metatarsals with the tarsal bones and the four dorsal basal ligaments unite to one another the bases of the metatarsals.
By far the strongest ligament of the sole of the foot is the long plantar ligament. It arises from the whole of the under surface of the calcaneus and from the medial and lateral tuberosities of the tuber calcanei, covering the entire width of the bone, and passes with very strong longitudinal fibres to the tuberosity of the cuboid. From this principal portion of the ligament superficial slips pass out, which pass over the tendon sheath of the groove on the cuboid and reach the basis of the lateral metatarsals. They form the retinaculum for the tendon sheath of the Peroneus longus.
Almost as strong is the plantar calcaneo-navicular ligament. It runs with oblique, very strong fibres between the sustentaculum tali and the navicular. On its dorsal surface it contains the navicular fibrocartilage, which forms part of the socket for the head of the talus.
The plantar naviculari-cuneiform ligaments unite the navicular and the cuneiforms; the plantar cuboideo-navicular the cuboid and the navicular; the plantar cuneo-cuboid, the cuboid and the lateral cuneiform; and the plantar intercuneiform, the three cuneiforms with one another. In addition, there are plantar tarso-metatarsal and three plantar basal ligaments which correspond with the dorsal. The plantar calcaneo-cuboid ligament, which reinforces the capsule of the calcaneo-cuboid joint, unites with the dorsal surface of the long plantar ligament.
Those ligaments that are on neither the dorsal nor the plantar surfaces, but connect adjacent surfaces of the tarsal and metatarsal bones, are termed interosseous ligaments. In addition to the interosseous talo-calcaneal ligaments there is an interosseous cuneo-cuboid, interosseous intercuneiform, interosseous cuneo-metatarsal (especially between the medial cuneiform and the base of the second metatarsal where an interosseous basal ligament is wanting), and interosseous basal ligaments.
The metatarso-phalangeal and interphalangeal articulations of the foot are, with slight differences, similar to those of the hand, and present the same ligaments. The meta-tarso-phalangeal joint of the great toe shows a special structure in that two large sesamoid bones are imbedded in its capsule on the plantar surface.
The Trapezius arises from the squamous portion of occipital above the superior nuchal line, from the lig. nuchae, and from the spines of the last cervical and all the thoracic vertebrae. It is inserted into the acromial third of the clavicle, the acromion and spine of the scapula. Nerve: The spinal accessory (and branches of the cervical plexus). Action: The upper fibres raise the scapula, the lower depress it; all acting together draw the scapula backward; those to the skull rotate the head toward the opposite side, the lower fibres draw the lower angle of the scapula medialwards.
The Latissimus dorsi arises from the spinous processes of the lower six thoracic and all the lumbar vertebrae, from the dorsal surface of the sacrum, and the lateral lip of the iliac crest. Accessory slips arise from the lower three or four ribs and frequently from the lower angle of the scapula. It inserts into the crest of the lesser tuberosity of the humerus, together with the teres major from which it is separated by a bursa. Nerve: The thoraco-dorsal from the brachial plexus. Action: It draws the arm backward, adducts it and rotates it inward.
The Rhomboideus major arises from the spinous processes of the upper four thoracic vertebrae and inserts into the vertebral border of the scapula, below the spine.
The Rhomboideus minor arises from the lig. nuchae and the spinous process of the last cervical vertebra and is inserted into the vertebral border of the scapula, above the spine. Nerve: Both rhomboids are supplied by the dorsal scapular from the brachial plexus. Action: They draw the scapula towards the vertebral column and upwards.
The Levator scapulae arises by four heads from the posterior tubercles of the transverse processes of the four upper cervical vertebrae and inserts into the medial angle of the scapula. Nerve: The cervical plexus and the dorsal scapular. Action: Draws the medial angle of the scapula upwards and medially.
The Superior serratus posterior arises from the spinous processes of the two lower cervical and the two upper thoracic vertebrae and is inserted into the second to the fifth ribs, lateral to their angles.
The Inferior serratus posterior arises, through the posterior layer of the lumbodorsal fascia, from the spinous processes of the lower thoracic and upper lumbar vertebrae. It inserts into the lower borders of the four lower ribs. Nerve: Both serrati are supplied by intercostal nerves. Action: They act on the ribs in inspiration.
The Splenius capitis arises from the lig. nuchae and the spinous processes of the last cervical and first thoracic vertebrae and inserts into the lateral half of the superior nuchal line, as far out as the mastoid process. Nerve: The posterior branches of the 1-4 (5) cervical nerves. Action: Both muscles draw the head backwards; acting singly, they rotate the head to the same side.
The Splenius cervicis arises from the spinous processes of the third or fourth to the sixth thoracic vertebra and is inserted into the posterior tubercles of the transverse processes of the upper three cervical vertebrae. Nerve: The posterior branches of cervical nerves. Action: Draws the head backwards and rotates the upper cervical vertebrae and head to the same side.
The Spino-transversalis consists of the lateral Ilio-costalis and the medial, stronger Longissimus. Medial to the latter and fused with it is the Spinalis.
The Iliocostalis has three parts which pass over into one another without any sharp lines of demarcation. The Iliocostalis lumborum arises with the Longissimus dorsi from the dorsal surface of the sacrum and from the lateral lip of the iliac crest. It inserts into the angles of the fifth to the twelfth ribs. The Iliocostalis arises by digitations from the twelfth to the seventh ribs and inserts into the angles of the upper six ribs and the transverse process of the seventh cervical vertebra. The Iliocostalis cervicis arises from the upper and middle ribs and inserts into the transverse processes of the middle cervical vertebrae. Nerves: Posterior branches of the cervical, thoracic and lumbar nerves. Action: Extends the vertebral column and bends it backward, acting with the other long muscles.
The Longissimus also consists of three parts. The Longissimus dorsi arises with the iliocostalis lumborum from the dorsal surface of the sacrum and from the spinous processes of the lumbar and lower thoracic vertebrae. It inserts into the accessory processes of the upper lumbar and the transverse processes of the thoracic vertebrae, and, more laterally, into the tip of the transverse processes of the lumbar vertebrae and into all the ribs, between their angles and tubercles. The Longissimus cervicis is not clearly separated from the upper part of the Longissimus dorsi; it arises from the transverse processes of the upper thoracic vertebrae and inserts into the transverse processes of the upper and middle cervicals.
The Longissimus capitis (Trachelomastoid) arises from the transverse processes of the upper thoracic vertebrae and from the transverse and articular processes of the middle and lower cervicals. It is inserted into the posterior border of the mastoid process. Nerves : Posterior rami of the cervical and thoracic nerves. Action: Extends the vertebral column and bends it backwards; the Longissimus capitis acts also on the neck and head.
The Spinalis again has three portions. The Spinalis dorsi arises from the spinous processes of the upper lumbar and the lower thoracic and inserts into the same processes of the middle and upper thoracic vertebrae. The Spinalis Cervicis (inconstant) passes between the spinous processes of the lower cervical vertebrae and those of the upper thoracic. The Spinalis capitis is properly a portion of the Semispinalis capitis, representing its inconstant spinal head. Nerves: Posterior rami of the cervical, thoracic and lumbar nerves. Action: Bends the vertebral column sidewise; acting on both sides, it extends.
The Semispinalis has three portions. The Semispinalis dorsi and cervicis arise from the transverse processes of the thoracic and lower cervical vertebrae and, passing steeply upward and inward, inserts into the spinous processes of the middle and upper thoracic and lower cervical vertebrae. The lateral portion of the Semispinalis capitis arises from the transverse processes of the third cervical to the fifth or sixth thoracic vertebrae, the medial portion (the spinalis capitis) from the spinous process of the upper thoracic and lower cervical vertebrae. Its insertion is into the squamous portion of the occipital, between the superior and inferior nuchal lines. Nerves: Posterior rami of the cervical and thoracic nerves. Action: Extends the vertebral column and head. Acting on one side only it rotates the head toward the opposite side.
The Multifidus is a series of small muscles that arise from the dorsal surface of the sacrum and the transverse processes of all the vertebrae up to the lower cervical and pass upwards and inwards to the second or third spinous process next above.
The Rotatores longi and breves pass between the bases of the transverse processes of the thoracic vertebrae and the spinous process of the vertebra next (breves), or next but one (longi), above. Nerves: The Multifidus and Rotatores are supplied by the posterior rami of the spinal nerves. Action: Extension of the spinal column and rotation the opposite side.
The Rectus capitis posterior major arises from the spinous process of the axis (epistropheus) and is inserted into the inferior nuchal line. The Rectus capitis posterior minor arises from the posterior tubercle of the atlas and ascends to the inferior nuchal line. The Rectus capitis lateralis (see Fig. A276) takes its origin from the transverse process of the atlas and passes to the jugular process of the occipital.
The Obliquus capitis superior arises from the transverse process of the atlas and passes upwards to the inferior nuchal line. The Obliquus capitis inferior arises from the spinous process of the axis (epistropheus) and passes outwards and upwards to the transverse process of the atlas.
Nerve : All five muscles are supplied by the suboccipital nerve, the posterior ramus of the first cervical. Action: They serve for the extension and rotation of the head. The Obliquus inferior and Rectus major and minor rotate toward the same side, the Obliquus superior to the opposite one; the Rectus lateralis bends the head forward.
The Interspinales are wanting in the thoracic region. Elsewhere they extend from spinous process to spinous process. The first are between the atlas and axis (epistropheus), and throughout the cervical region they are paired, the spinous processes being bifurcated.
The Intertransversarii are, as a rule, absent in the thoracic region. In the cervical there are Anterior intertransversarii between the anterior tubercles of successive vertebrae, and Posterior intertransversarii between successive posterior tubercles. In the lumbar region there are Medial intertransversarii, between the accessory and mamillary processes of succeeding vertebrae, and Lateral intertransversarii between the transverse processes; the latter are much the larger.
Nerves: Posterior rami of the spinal nerves. Action: The interspinales bend the spinal column backwards, the intertransversarii bend it laterally.
The Levatores costarum are really the posterior portions of intercostal muscles. They arise from the transverse processes of the thoracic vertebrae and pass to the succeeding rib (Levatores costarum breves), or to the next but one (Levatores costarum longi) inserting between the tuberosity and the angle. Action: Raise the ribs, extend the vertebral column and bend it laterally.
The strongest fascia of the back is the lumbo-dorsal fascia whose relations are shown in Fig. A255. The superficial layer of muscles is covered by the general fascia, but the different layers of the long muscles are not distinctly separated by fascia and the short muscles are destitute of it.
The Pectoralis major arises by a clavicular portion from the sternal half of the clavicle, by a sterno-costal portion from the anterior surface of the manubrium and body of the sternum and from the second to the sixth costal cartilages and by an abdominal portion from the abdominal aponeurosis (sheath of the Rectus). It is inserted by a broad tendon, resembling a two-layered pouch with the opening upward, into the crest of the great tuberosity of the humerus. Nerve: The anterior thoracic from the brachial plexus. Action: Adducts the arm, draws it medially and forward, rotates it inwards.
The Pectoralis minor arises from the second to the fifth ribs, near the cartilages, and inserts into the apex of the coracoid process of the scapula. Nerve: The anterior thoracic from the brachial plexus. Action: Draws the scapula downwards; if the scapula is fixed it raises the ribs.
The Subclavius is a small muscle arising from the first costal cartilage and inserting into the under-surface of the acromial end of the clavicle. Nerve: The subclavian from the brachial plexus. Action: Fixes the clavicle in the sterno-clavicular joint, drawing it forward and downward.
Serratus anterior arises by digitations from the first to the ninth ribs. The upper portion, from the first and second ribs, is inserted into the medial angle of the scapula; the middle portion, from the second and third ribs, into almost the entire length of the vertebral border of the scapula; the lower portion, from the fourth to the ninth rib, converges on the inferior angle of the scapula. Nerve: The long thoracic from the brachial plexus. Action: Draws the scapula forward and laterally, especially its lower angle, the scapula thus being rotated on the chest wall, as in raising the arm.
The Obliquus externus arises by seven or eight digitations from the fifth or sixth to the twelfth rib. It is inserted into the lateral lip of the iliac crest and into the inguinal ligament and the anterior wall of the sheath Rectus. Nerve: The lower intercostal nerves and branches from the lumbar plexus, the ilio-hypogastric and ilio-inguinal. Action: Compresses the abdomen, draws the trunk forward or rotates it to the same side, raises the pelvis.
The Obliquus internus arises from the intermediate line of the iliac crest, from the lumbo-dorsal fascia and from the lateral two-thirds of the inguinal ligament. It is inserted into the lower borders of the last three ribs and the linea alba, its tendon forming the anterior wall of the sheath of the Rectus and the upper part of its posterior wall. Nerves: The lower intercostals and branches of the lumbar plexus (ilio-hypogastric, ilio-inguinal and genito-femoral). Action: Similar to that of the external oblique.
The Cremaster arises from the lower bundles of the Internal oblique and from the anterior wall of the sheath of the Rectus, and is continued down over the spermatic cord to the scrotum. Nerve: External Spermatic. Action: Draws the testis upwards.
The Transversus arises from the inner surfaces of the last six ribs (fleshy), from the lumbodorsal fascia (tendinous) and from the inner lip of the iliac crest and the lateral third of the inguinal ligament (fleshy). It is inserted at the linea semilunaris into the posterior wall of the sheath of the Rectus and, below, into the anterior wall. Nerves: The lower intercostals and branches from the lumbar plexus (iliohypogastric, ilioinguinal, and genito-femoral). Action: Compresses the abdomen.
The Rectus abdominis arises from the cartilages of the fifth to the seventh rib and from the xiphoid process, and inserts by a short tendon into the upper border of the pubis between the tubercle and the upper border of the symphysis. The muscle fibres are interrupted by tendinous inscriptions, of which three are constant; an upper, in the region of the costal arch; a lower in the neighborhood of the umbilicus; and a middle between these. A fourth sometimes occurs below the umbilicus and usually only in the lateral part of the muscle. At the inscriptions the muscle unites with the anterior wall of its sheath, from which elsewhere it is separated by loose connective tissue. The posterior wall does not unite with the inscriptions; it ends below at the semicircular line (Douglas' line), not always very distinct, the lower part of the muscle having behind it only the fascia transversalis. Nerves: The middle and lower intercostals and occasionally the first lumbar. Action: It bends the trunk forward or raises the pelvis; it also aids in compressing the abdominal contents.
The Pyramidalis is an inconstant muscle that arises immediately in front of the origin of the Rectus. It is inserted into the linea alba above the symphysis. Nerves: The lower intercostals. Action: Tenses the linea alba.
In the aponeurosis of the Obliquus abdominis externus a triangular cleft occurs, no fibres inserting between the pubic tubercle and the upper border of the symphysis. The lateral angle of the cleft is rounded off by superficial, arched intercrural fibres, and the medial angle by the reflexed inguinal ligament, extending upwards from the insertion of the inguinal ligament. The irregularly quadrangular opening so formed is the subcutaneous inguinal ring, through which the spermatic cord passes in the male and the ligamentum teres of the uterus in the female (see Fig. A262). The borders of the aponeurosis that bound the ring are termed the crura (superius and inferius).
The tendon of the Obliquus internus forms both walls of the sheath (vagina) of the Rectus, which is strengthened in front by the Obliquus externus and behind by the Transversus. In the lower third of the abdomen the posterior wall is completely wanting below the semicircular line (Douglasi) (see here), all three muscles passing to the anterior wall. In the middle line the sheaths of the two Rectus muscles unite to form a broad, tendinous strip, the linea alba, that extends from the xiphoid process to the upper border of the symphysis pubis (see Fig. A266).
The Quadratus lumborum arises from the medial lip of the iliac crest, the iliolumbar ligament and the transverse processes of the lower lumbar vertebrae. Its fibres form two parallel layers which are partly interwoven. It inserts into the medial half of the twelfth rib and into the transverse processes of the upper and middle lumbar vertebrae. Nerves: Branches from the lumbar plexus and the twelfth intercostal. Action: Draws the last rib downwards and bends the lumbar vertebrae laterally.
The Diaphragm arises by its sternal portion from the xiphoid process of the sternum, by its costal portion from the inner surface of the last six ribs and their cartilages, and by its lumbar portion from the lumbar vertebrae by three pairs of crura. The medial crura are attached to the anterior surface of the third and fourth vertebrae, the intermediate crura to the lateral surfaces of the body of the second vertebra and the lateral crura to the transverse processes of the first vertebra and to the lumbo-costal arches. From these origins the fibres radiate to a trifoliate central tendon. Between the medial crura is the aortic opening (hiatus); in the muscular part of its lumbar portion, the oesophageal opening; and in the central tendon, the foramen for the vena cava. Between the medial and intermediate crura and between the latter and the lateral there are gaps, and also between the costal and sternal portions. Nerve: Phrenic from the cervical plexus. Action: A muscle of respiration, inspiratory.
The Iliopsoas consists of two or three parts, the Psoas major, Psoas minor, and Iliacus. The Psoas major arises from the upper and lower borders of the bodies of the twelfth thoracic to the fourth lumbar vertebra, and from the fibrocartilages between these; also from the transverse processes of all the lumbar vertebrae. The Psoas minor is inconstant; when present it arises from the bodies of the last thoracic and first lumbar vertebrae and is inserted by a long slender tendon into the iliac fascia and the iliopectineal eminence. The Iliacus arises from the whole of the iliac fossa. It unites with the psoas major, and the combined muscle passes over the crest of the pubis and over the capsule of the hip joint, separated from this by the iliopectineal bursa, and inserts into the lesser trochanter of the femur. Nerves: Branches from the lumbar plexus. Action: Flexes the thigh, rotates it inwards and aids in adduction. The Psoas minor tenses the iliac fascia.
The External intercostals pass between the opposed borders of successive ribs, beginning behind the tuberosity and ending in front shortly before the junction of the ribs and their cartilages. Their fibres are directed from above downwards and inwards, like those of the External oblique. In the region of the costal cartilages they are continued as tendinous bundles, the external intercostal ligaments.
The Internal intercostals are covered by the external, except in the region of the cartilages. Their fibres are directed upwards and inwards, like those of the Internal oblique, and are lacking at the hinder ends of the ribs, between the angles and the tuberosities, where they are replaced by the internal intercostal ligaments.
The Subcostales immediately succeed the Internal intercostals. They are not quite constant and differ from the Internal intercostals in that they occur at the hinder portions of the ribs and pass over one or more. They occur only on the lower ribs and are usually largely tendinous.
The Transversus thoracis (triangularis sterni) arises from the posterior surface of the body of the sternum and the xiphoid process and is inserted into the inner surfaces of the cartilages of the second (third) to the sixth rib.
Nerves: The Intercostals are supplied by the intercostal nerves which run between the external and internal. The Transversus thoracis and Levatores costarum are also supplied by these nerves. Action: The Intercostals are respirator muscles; the externals and the portions of the internals between the costal cartilages serve in inspiration, as do also probably the rest of the Intercostals and the Subcostals, though they have been held to act in expiration.
For the Levatores costarum see here.
The pectoral fascia, which covers the Pectoralis major and Serratus anterior, is merely a portion of the general fascia and as such is continued downwards over the superficial abdominal muscles and backwards over the dorsal muscles (Latissimus). Directly continuous with it is the axillar fascia, perforated by numerous blood vessels. an in part much stronger sheet, the coraco-clavicular fascia lies between the Pectoralis major and Pectoralis minor, covering the Subclavius and the axillary vessels. It is especially strong where it rests on the Subclavius, and is attached to the under surface of the clavicle and to the coracoid process. The endothoracic fascia covers the inner surfaces of the ribs and Intercostal muscles and also the upper surface of the Diaphragma; it is in contact with the parietal layer of the pleurae.
The superficial layer of the abdominal muscles is covered by the general fascia, but this, in the region of the inguinal ring in the lower region of the abdomen, acquires a very considerable strength and is continued as the cremasteric fascia (Cooper's) upon the spermatic cord. It is also continuous with the fascia penis and forms the ligamentum fundiforme penis (in the female the much weaker ligamentum fundiforme clitoridis) which arises from the linea alba, to which the fascia is closely united, and, dividing into two portions, surrounds the root of the penis; it is rich in elastic fibres. The sheath of the Rectus serves as its fascia. The inner surface of the Transversus, the anterior surface of the Quadratus lumborum and the posterior surface of the posterior wall of the sheath of the Rectus are covered by the transversalis fascia. Over these structures the fascia is especially strong and it is firmly fused with the tendinous portion of the Transversus and the posterior wall of the sheath of the Rectus. Below the linea semicircularis it alone forms the posterior wall of the sheath. Above the symphysis it fuses with a triangular, tendinous offset from the superior pubic ligament, the adminiculum lineae albae. At the inguinal ligament, with which it unites, the Transversalis passes over into the iliopectineal fascia and it also passes over into that portion of the iliac fascia that covers the anterior surface of the Psoas. Above it is lost on the under surface of the Diaphragm. It is in contact with the parietal layer of peritoneum.
The Platysma arises from the skin covering the pectoral and deltoid fasciae and is inserted into the skin over the base of the mandible, the chin and face. Nerve: Ramus colli of the facial nerve. Action: contracts the skin of the neck and upper part thorax and tenses the cervical fascia.
The Sterno-mastoid (sterno-cleido-mastoid) arises by a sternal head from the anterior surface of the manubrium sterni and by a clavicular head from the sternal end of the clavicle. It is inserted into the lateral part of the base of the mastoid process and the lateral half of the superior nuchal line. Nerve: The spinal accessory. Action: Fixes the head, turns the face upwards. If only one acts, the head is drawn to the same side and rotated towards the opposite one.
The Sterno-hyoideus arises from the upper border of the first costal cartilage, the posterior surface of the manubrium and the sterno-clavicular joint. It has frequently a tendinous inscription in its lower part and inserts into the body of the hyoid bone.
The Sterno-thyreoideus arises from the inner surface of the first costal cartilage and from the posterior surface of the manubrium. It also frequently has a tendinous inscription in its lower part, and inserts into the outer surface of the thyreoid cartilage.
The Thyreo-hyoideus arises from the outer surface of the thyreoid cartilage and is inserted into the lateral third of the body of the hyoid and into the root of the greater cornu. The Omohyoideus arises from the upper border of the scapula between the medial angle and the scapular notch. It is divided in the middle of its course into two bellies by an intervening tendon, and is inserted into the lower border of the lateral part of the body of the hyoid.
Nerves: All four muscles are supplied from the ansa hypoglossi. The Thyreo-hyoideus usually has a direct branch from the hypoglossal. Action: Draw the hyoid bone and larynx downwards and assist in swallowing. The Omohyoideus by the union of its intermediate tendon with the cervical fascia, tenses that fascia.
The Digastricus is divided into two bellies by an intermediate tendon which is attached to the hyoid bone. The posterior belly (venter) arises from the notch on the mastoid process and the anterior belly is attached to the digastric fossa of the mandible. Nerves: The anterior belly is supplied by the mylohyoid and the posterior by the facial. Action: Opens the mouth, raises and fixes the hyoid bone.
The Stylo-hyoideus arises from the styloid process of the temporal and is inserted by two slips into the anterior and posterior borders of the lateral part of the hyoid. The intermediate tendon of the digastric passes between the two slips of insertion. Nerve: The facial. Action: Fixes the hyoid, drawing it upward and laterally.
The Mylo-hyoideus arises from the mylohyoid line of the mandible. The muscle forms the floor of the mouth extending across the arch of the mandible. Its more median fibres unite in a median raphe; the lateral insert into the upper border of the body of the hyoid. Nerve: The mylohyoid from the third division of the trigeminus. Action: Raises the floor of the mouth, depresses the mandible, aids in deglutition.
Th Genio-hyoideus arises from the mental spine and inserts into the anterior border of the body of the hyoid. Nerve: Hypoglossal. Action: Aids the Mylohyoid, fixes the hyoid, and depresses the mandible.
The Scalenus anterior arises from the anterior tubercles of the transverse processes of the third (fourth) to the sixth cervical vertebrae and is inserted into the scalene tubercle of the first rib.
The Scalenus medius arises from the anterior tubercles of the transverse processes of all the cervical vertebrae. It is inserted into the first rib, lateral to the preceding. The Scalenus posterior arises from the posterior tubercles of the transverse processes of the fifth to the sixth (seventh) cervical vertebrae and inserts into the upper border of the second rib.
Nerves: From the cervical and brachial plexuses. Action: Elevate the upper two ribs. Muscles of respiration.
The Longus colli arises by a medial limb from the bodies of the upper thoracic and lower cervical vertebrae; by an upper lateral limb from the anterior tubercles of the transverse processes of the upper cervical vertebrae; and by a lower lateral limb from the lateral surfaces of the bodies of the upper thoracic vertebrae. It inserts by its medial limb into the bodies of the upper cervical vertebrae; by its upper lateral limb into the anterior tubercle of the atlas and the bodies of the succeeding vertebrae; and by its lower lateral limb into the transverse processes of the lower cervical vertebrae, especially the sixth.
The Longus capitis arises from the anterior tubercles of the transverse processes of the third to the sixth cervical vertebrae and inserts into the lower surface of the basilar portion of the occipital.
The Rectus capitis anterior has its origin from the root of the transverse process of the atlas and is inserted close to the preceding muscle. Nerves: Special branches of the cervical plexus. Action: Bend the vertebral column and head anteriorly; acting singly bend the head to the same side.
The facial muscles include the Epicranius with the associated auricular muscles, the Orbicular muscle of the eyelids, the muscles of the mouth and those of the nose.
The differ from most of the other skeletal muscles in many respects; they are in the deeper layers of the skin, they generally lack fascia, they are entirely fleshy or have very short tendons. In certain regions they form sphincters. Frequently adjacent muscles are imperfectly separated; thus the muscles of the mouth region unite together in the upper and lower lip.
The epicranial muscles are attached to a common tendinous sheet, the galea aponeurotica, which covers the whole vault of the skull.
The Frontalis arises from the upper border of the orbit and is attached above to the galea aponeurotica.
The Procerus is attached to the nasal bones and is inserted into the skin over the glabella.
The Occipitalis arises from the supreme nuchal line and passes to the galea aponeurotica.
The Epicranius auricularis is a superficial muscle that is divided by the branches of the superficial temporal artery into three parts, which are quite distinct from the deeper Auriculus anterior and posterior and do not all reach the auricular cartilage.
Nerve: The facial. Action: Move the scalp.
The Auricularis anterior (attrahens) arises from the superficial temporal fascia and from the margin of the galea aponeurotica; the Auricularis superior (attollens) arises from the galea aponeurotica in the temporal region; and the Auricularis posterior (retrahens) from the tendon of insertion of the sterno-mastoid. The three muscles insert into the root of the auricular cartilage. Nerve: The facial. Action: Move the auricle.
The Orbicularis oculi has three portions: The orbital portio arise the frontal process of the maxilla at the medial angle of the orbit and its fibres surround the opening of the orbit like a sphincter; some of the fibres insert into the eyebrow (depressor capitis supercilii). The palpebral portion has its origin in the medial palpebral ligament and inserts into the lateral palpebral raphe, while the lacrimal portion (Horner's muscle) is attached medially to the posterior lacrimal crest and fuses laterally with the palpebral portion. A portion arising from the nasal part of the frontal bone and inserting into the skin of the eyebrow is termed the Corrugator supercilii. Nerve: The facial. Action: Closes the eyelids, compresses the lacrimal sac.
The Quadratus labii superioris arises by three heads. The angular head arises from the frontal process of the maxilla and passes partly to the ala of the nose and partly to the upper lip. The infraorbital head arises from the infraorbital border and the zygomatic head from the malar surface of the zygomatic bone; these two heads pass to the upper lip.
The Zygomaticus arises from the malar surface of the zygomatic bone and passes to the angle of the mouth.
Nerve: The facial. Action: Movement of the upper lip, the ala of the nose and the angle of the mouth.
The Risorius, usually part of the Platysma or of the Triangularis, arises from the parotideo-masseteric fascia and passes to the angle of the mouth.
The Triangularis (depressor anguli oris) arises from the anterior end of the base of the mandible and passes to the angle of the mouth and the lower lip.
The Caninus (levator anguli oris) arises from the canine fossa of the maxilla and passes to the upper lip and the angle of the mouth.
The Quadratus labii inferioris arises from the anterior part of the base of the mandible and passes to the lower lip.
The Incisivus labii superioris arises from the jugum of the upper lateral incisor tooth and passes to the upper lip. The Incisivus labii inferioris arises from the jugum of the lower lateral incisor tooth and passes to the lower lip. The Incisive muscles probably should not be regarded as distinct muscles any more than the slip of the Nasalis that passes to the cartilaginous septum of the nose (Depressor septi).
The Bucinator arises from the bucinator crest of the mandible, the posterior end of the alveolar process of the maxilla and the pterygo-mandibular raphe. Its fibres at the angle of the mouth are continued into the upper and lower lips, arching around the mouth to form the Orbicularis oris.
The Mentalis (levator menti) arises from near the jugum of the lower medial incisor tooth and passes to the skin of the chin.
Nerve: The facial. Action: Move the lips, cheeks and chin.
The Nasalis consists of two portions, a transverse portion arising from the maxilla and passing transversely to the bridge of the nose, and an alar portion from the jugum of the upper canine tooth to the ala of the nose and the septal cartilage. Nerve: The facial. Action: Slight movement of the nose, especially of the ala.
The Masseter arises by its superficial fibres from the lower border of the zygoma, by its deeper fibres from the posterior part of the lower border and from the inner surface of the zygoma. It is inserted into the lateral surface of the ramus of the mandible from the mandibular notch to the angle (masseteric tuberosity). Nerve: The masseteric nerve from the third division of the trigeminus. Action: Closes the jaws.
The Temporalis arises from the temporal fossa, below the inferior temporal line, and from the deep lamina of the temporal fascia. It inserts into the apex and medial surface of the coronoid process of the mandible. Nerves: The deep temporal nerves from the third division of trigeminus. Action: Closes the jaws.
The Pterygoideus externus arises by its chief head from the lateral surface of the lateral plate of the pterygoid process and from the tuberosity of the maxilla; by its accessory head from the infratemporal crest of the greater wing of the sphenoid. It is inserted into the pterygoid fovea on the condyloid process of the mandible and into the articular disk of the mandibular articulation. Nerve: The external pterygoid from the third division of the trigeminus. Action: Draws the mandible forward. By the alternate action of the two muscles lateral movements of the mandible are produced.
The Pterygoideus internus arises from the pterygoid fossa, from the pyramidal process of the palatine and from the medial surface of the lateral plate of the pterygoid process. It inserts into the medial surface of the angle of the mandible (pterygoid tuberosity). Nerve: The internal pterygoid from the third division of the trigeminus. Action: Closes the jaws.
Over the vault of the skull there is no fascia, since the galea aponeurotica is directly connected with the deeper layers of the skin.
The parotideo-masseteric fascia is a sheet that passes over the parotid gland and the Masseter muscle. At the zygoma it is continuous with the temporal fascia, at the anterior border of the Masseter with the bucco-pharyngeal and at the angle of the mandible with the cervical (Fig. A264).
The temporal fascia is the strongest fascia of the head. It extends as a dense membrane from the superior temporal line to the zygoma and at about the middle of its course it splits into two laminae, a superficial and a deep, between which there is some fat tissue. The interval between the two laminae increases downwards, the superficial lamina inserting into the lateral and the deep into the medial border of the zygoma. At its upper edge it is connected with the galea aponeurotica.
The bucco-pharyngeal fascia rests in its anterior part on the bucinator muscle and is connected with the parotideo-masseteric fascia; its posterior part is stronger and covers the inner surface of the Internal pterygoid muscle. It is in this that the pterygo-mandibular raphe and stylo-mandibular ligament are developed. This posterior part of the fascia bounds the lateral posterior wall of the mouth cavity and the lateral wall of the pharynx (see here).
In the neck the fascia colli (cervical fascia) and the praevertebral fascia may be distinguished. The former is divided into a superficial and a deep lamina, this latter being sometimes termed the middle layer. The former covers the superficial muscles of the neck and also the larynx, trachea and submaxillary gland, but is of variable strength in its different parts, being very thin over the lateral surface of the Sternomastoid. At the anterior border of the Trapezius it passes into the fascia of the back of the neck. The deep, distinctly stronger lamina covers the Omohyoid and the posterior surfaces of the other infrahyoid muscles and, anterior to the larynx and trachea, fuses with the superficial lamina. The quite distinct praevertebral fascia covers the anterior surface of the praevertebral muscles and the bodies of the cervical vertebrae, where these are uncovered by muscles; it is strong and partly tendinous.
The Supraspinatus arises from the supraspinous fossa of the scapula and is inserted into the upper facet of the greater tuberosity of the humerus. The Infraspinatus arises from the lower border of the spine of the scapula, from the infraspinous fossa and the infraspinatus fascia. It inserts into the middle facet on the greater tuberosity of the humerus. Nerve: The subscapular from the brachial plexus. Action: The Supraspinatus abducts the arm; the Infraspinatus rotates it outwards.
The Teres minor arises from the lower part of the infraspinous fossa, from about two-thirds of the lateral border of the scapula and from the infraspinatus fascia. It inserts into the lower facet of the greater tuberosity of the humerus. Nerve: The axillary from the brachial plexus. Action: External rotation of the arm.
The Teres major arises from the middle third of the axillary border of the scapula and has a tendinous insertion into the crest of the lesser tuberosity of the humerus. Its tendon is posterior to that of the Latissimus dorsi, from which it is separated by a bursa. Nerves: The lower subscapular from the brachial plexus. Action: Assists the Latissimus (see here), rotates the arm inwards.
The Subscapularis arises from the subscapular fossa and its muscular lines and inserts by a strong tendon on the lesser tuberosity of the humerus and the upper part of its crest. A subscapular bursa, between the tendon and the capsule of the shoulder joint, communicates with the latter. Nerves: Subscapular nerves from the brachial plexus. Action: Internal rotation and adduction of the arm.
The Deltoid arises from the acromial third of the clavicle, from the acromion and the spine of the scapula. It is inserted into the deltoid tuberosity of the humerus, a subdeltoid bursa being interposed between its tendon and the bone. Nerve: The axillary. Action: Abducts the arm to the horizontal position.
Eleven muscles of the trunk are attached to the skeleton of the upper limb, especially to the shoulder girdle. These are:
The large Triceps is the only muscle of the extensor surface of the upper arm, covering its entire surface and being continued upon the forearm as the Anconaeus. It takes origin by three heads. The long head arises from the infraglenoid tuberosity of the scapula; the lateral head from the lateral and posterior portions of the upper part of the shaft of the humerus, below the greater tuberosity, and also from the upper two-thirds of the lateral intermuscular septum; the medial head from the whole length of the medial intermuscular septum down to the medial epicondyle, from the posterior surface of the humerus below the crest of the great tuberosity, following the groove for the radial nerve, and from the lateral intermuscular septum down to the lateral epicondyle. From these three heads the fibres concentrate to a broad tendon that is attached to the posterior part of the upper surface of the olecranon, fibres also passing to the antebrachial fascia.
The Anconaeus is in close relation to the lower part of the medial head of the triceps. It arises from the lateral epicondyle of the humerus and inserts into the dorsal surface of the ulna, immediately below the olecranon. Nerve: The radial supplies both muscles. Action: Extension of the forearm.
The Biceps brachii has two heads of origin. The long head arises from the supraglenoid tuberosity of the scapula and the short head from the tip of the coracoid process. The two heads unite to form a common tendon which is inserted into the tuberosity of the radius and by means of the lacertus fibrosus into the antebrachial fascia. A bicipito-radial bursa lies between the tendon and the radius. Nerve: The musculo-cutaneus. Action: Supinates and flexes the forearm, tenses the antebrachial fascia; the long head abducts, the short head adducts the arm.
The Coraco-brachialis arises together with the short head of the Biceps from the tip of the coracoid process. It is inserted into the anterior and medial surfaces of the humerus, below the crest of the lesser tuberosity, and into the medial intermuscular septum. Nerve: The musculo-cutaneus, which pierces it. Action: Aids in raising the arm and in its adduction.
The Brachialis arises from the lower parts of the anterior and medial surfaces of the humerus, from the lateral surface below the deltoid tuberosity, and from the medial and lateral intermuscular septa almost down to the epicondyles. It passes over the anterior surface of the capsule of the elbow joint and is inserted into the tuberosity of the ulna. Nerve: The musculo-cutaneus and frequently also a branch from the radial. Action: Flexor of the forearm.
Between the flexor and extensor muscles there is, in the lower portion of the upper arm, on either side an intermuscular septum. The stronger medial one ends at the medial epicondyle, the much weaker lateral at the lateral epicondyle. They serve for the origin of both groups of muscles, the lateral also for that of the radial group.
The long head of the Triceps passes between the Teres major and Teres minor and divides the interval between these two muscles into a lateral quadrangular space, through which pass the axillary nerve and the posterior circumflex artery, and a medial triangular one, which gives passage to the circumflex scapular artery.
The medial head at the intermuscular septum adjoins the Brachialis and at the medial epicondyle the Anconaeus, which continues its fibre-course. The lateral head at the lateral intermuscular septum adjoins from above downwards, the Brachialis, the Brachio-radialis and sometimes also the Extensor carpi radialis longus.
The superficial layer of the flexor muscles of the forearm arises by a common tendon from the medial epicondyle of the humerus. All the muscles of the group, except the Pronator teres, pass over the wrist joint and have more or less long tendons. They occupy the ulnar side of the volar surface of the forearm and in their upper portions are firmly attached to the antebrachial fascia. A deep furrow separates them above from the muscles of the radial group, and in this groove the biceps tendon descends to its insertion.
The Pronator teres arises by a humeral head from the medial epicondyle of the humerus and the antebrachial fascia and by an ulnar head from the coronoid process of the ulna. It inserts into the middle of the lateral surface of the radius. Nerve: Median, which passes between the two heads. Action: Pronation; assists also in flexion.
The Flexor carpi radialis arises from the medial epicondyle and the antebrachial fascia and is inserted into the volar surface of the base of the second metacarpal. Nerve: Median. Action: Volar flexion and radial abduction; also pronation.
The Palmaris longus is not always present. It arises from the medial epicondyle and the antebrachial fascia and inserts into the palmar aponeurosis and the transverse carpal ligament. Nerve: Median. Action: Tenses the palmar aponeurosis and assists in flexion. The Flexor digitorum sublimis arises from the medial epicondyle by a humeral head and from the volar surface and volar border of the radius by a radial head. It is inserted by four long tendons into the middle phalanges of the second to the fifth fingers. Nerve: Median. Action: Flexes the middle phalanges of the four ulnar fingers; assists in flexion of the forearm.
The Flexor carpi ulnaris arises by a humeral head from the medial epicondyle and by an ulnar head from the olecranon and, through the antebrachial fascia, from the upper two-thirds of the posterior border of the ulna. It inserts into the pisiform bone and, by means of the ligaments of that bone (Fig. A224), into the base of the fifth metacarpal. Nerve: Ulnar. Action: Volar flexion and ulnar abduction.
The deep layer of the flexor surface of the forearm is almost completely covered by the superficial layer and consists of two deep flexors of the fingers and the Pronator quadratus. Strictly speaking it represents two layers, since the two flexors completely cover the Pronator quadratus.
The Flexor digitorum profundus arises from the volar surface of the ulna and from the interosseous membrane. It divides into four long tendons which pass to the terminal phalanges of the second to the fifth fingers. Nerve: Ulnar for its ulnar portion and for its radial part the median. Action: Flexion of the terminal phalanges of the 2-5 fingers; assists in flexing the forearm.
The Flexor pollicis longus arises by a principal radial head from the volar surface of the radius, below the insertion of the supinator, and by an inconstant humeral head from the medial epicondyle. It is inserted into the terminal phalanx of the thumb. Nerve: The volar interosseous from the median. Action: Flexes the terminal phalanx of the thumb. The Pronator quadratus (see Fig. A300) passes across from the volar border of the ulna to the volar border and surface of the radius. Nerve: The volar interosseous from the median. Action: Pronation.
The Brachio-radialis arises from the lateral border of the humerus and from the lateral intermuscular septum of the upper arm and is inserted by a flat tendon into the upper end of the styloid process of the radius. Nerve: The radial (musculo-spiral). Action: Flexion of the forearm; if the arm is flexed, either pronation or supination.
The Extensor carpi radialis longus arises from the lower end of the lateral intermuscular septum and the lateral epicondyle of the humerus and inserts into the dorsal surface of the base of the second metacarpal. The Extensor carpi radialis brevis arises from the lateral epicondyle of the humerus and from the antebrachial fascia and is inserted into the dorsal surface of the base of the third metacarpal. Nerve: The radial (musculo-spiral). Action: The brevis especially gives dorsal flexion of the hand; the longus radial abduction; the latter supinates if the arm is extended, pronates if it is flexed.
The Extensor communis digitorum arises from the lateral epicondyle of the humerus and from the antebrachial fascia. Its four tendons, which are connected by tendinous slips, pass into the dorsal aponeurosis of the second to the fifth digits. The Extensor digiti quinti proprius also arises from the lateral epicondyle of the humerus and from the antebrachial fascia and is inserted into the dorsal aponeurosis of the fifth finger. Nerve:The deep radial. Action: Extend the fingers and indirectly the hand.
The Extensor carpi ulnaris is separated from the two preceding muscles by an intermuscular septum and arises, like them, from the lateral epicondyle of the humerus and from the antebrachial fascia. It is inserted into the dorsal surface of the base of the fifth metacarpal. Nerve: The deep radial. Action: Dorsal flexion of the hand and ulnar abduction.
The Abductor pollicis longus (abductor ossis metacarpalis) arises from the dorsal surface of the ulna, the interosseous membrane and the dorsal surface of the radius, and is inserted into the base of the metacarpal of the thumb, slips passing to the trapezium (greater multangular) and to the Abductor pollicis brevis. The Extensor pollicis brevis arises from the dorsal surface of the radius and the interosseous membrane and inserts into the basal phalanx of the thumb. Nerve: The deep radial. Action: Abduction and extension of the thumb; the Abductor may also abduct the entire hand and assist in supination.
The Extensor pollicis longus arises from the dorsal surface of the ulna and the interosseous membrane and is inserted into the terminal phalanx of the thumb. The Extensor indicis proprius arises from the same parts and inserts into the dorsal aponeurosis of the index finger. Nerve: The deep radial. Action: Extension of the thumb or index finger; the Extensor pollicis assists in abducting the thumb.
The Supinator arises from the lateral epicondyle of the humerus, the radial collateral and annular ligaments and the supinator crest of the ulna. It is pierced by the deep radial nerve and so divided into a superficial and a deep layer. It is inserted into the volar surface and border, the lateral surface and dorsal border of the radius, both above and below the tuberosity. Nerve: The deep radial. Action: Supination.
The flexor tendons in the palm of the hand are covered by a strong tendinous membrane, the palmar aponeurosis, which is usually the direct expansion of the tendon of the Palmaris longus. It is always united to the transverse carpal ligament and passes laterally and medially into the thenar and hypothenar fasciae. Small at the transverse carpal ligament, it broadens toward the fingers and sends off bands which are lost in the skin of the basal portions of the second to the fifth fingers. In addition to the longitudinal fibres there are transverse fasciculi, especially distally. These bound proximally the gaps between the bands passing to the fingers, through which gaps pass nerves and vessels for the adjacent sides of the individual fingers and also the tendons of the lumbrical muscles.
The Palmaris brevis arises from the ulnar border of the palmar aponeurosis and occasionally from the trapezium (greater multangular). It is usually formed of a number of separate bundles and is inserted into the skin of the hand on its ulnar border. Nerve: Superficial volar branch of the ulnar. Action: Tenses the skin of the hand on the ulnar side.
The Abductor digiti quinti arises from the pisiform bone and is inserted into the dorsal aponeurosis of the little finger. The Flexor digiti quinti brevis is inconstant. It arises from the transverse carpal ligament and the hamulus of the unciform (hamate) bone and is inserted into the basal phalanx of the fifth finger. The Opponens digiti quinti has the same origin as the preceding and inserts into the ulnar border of the fifth metacarpal. Nerve: The deep volar branch of the ulnar. Action: Indicated by their names.
The Abductor pollicis brevis, Opponens pollicis and the superficial head of the Flexor pollicis brevis form a superficial sheet of thenar muscles, and the deep head of the Flexor and the Adductor pollicis a deep layer.
The Abductor pollicis brevis arises from the transverse carpal ligament and receives a slip from the tendon of the Abductor pollicis longus. It inserts into the basal phalanx of the thumb. Nerve: Median. Action: Abducts the thumb and aids in opposing it.
The Opponens pollicis arises from the transverse carpal ligament and the trapezium (greater multangular) and is inserted into the whole of the radial border of the metacarpal of the thumb up to its capitulum. Nerve: Median. Action: Opposes the thumb and aids in abduction.
The Flexor brevis pollicis arises by its superficial head from the tuberosity of the trapezium (greater multangular) and from the transverse carpal ligament; by its deep head from the trapezium (greater multangular) at the bottom of the carpal canal. It is inserted into the radial sesamoid bone at the metacarpo-phalangeal joint of the thumb. Nerve: The median for the superficial head, the deep volar branch of the ulnar for the deep head. Action: Flexes the basal phalanx of the thumb.
The Adductor pollicis has two heads. The oblique head arises from the os magnum (capitate) and unciform (hamate) at the bottom of the carpal canal; the transverse head arises from the volar surface of the third metacarpal. The insertion is into the ulnar sesamoid bone of the metacarpo-phalangeal joint of the thumb. Nerve: Deep volar branch of the ulnar. Action: Adducts the thumb and helps to oppose it.
The Interossei lie in the intervals between the metacarpal bones. They insert by expanded tendons into the dorsal aponeurosis of the fingers on the basal phalanges. The dorsal Interossei arise each by two heads from the borders of adjacent metacarpal bones.
The First dorsal interosseus arises from the first and second metacarpal, the Second from the second and third, the Third from the third and fourth and the Fourth from the fourth and fifth. The first and second insert into the radial side of the dorsal aponeurosis of the second and third fingers and the third and fourth into the ulnar side of the aponeurosis of the third and fourth fingers. Nerve: Deep volar branch of the ulnar. Action: Abduction of the fingers. Extension of the two distal phalanges and flexion of the basal ones.
The Interossei volares arise each by a single head, the first from the ulnar border of the second metacarpal, the second from the radial border of the fourth and the third from the radial border of the fifth. The first inserts into the ulnar side of the dorsal aponeurosis of the second finger, the second and third into the radial sides of the fourth and fifth fingers. Nerve: Deep volar branch of the ulnar. Action: Adduction of the fingers. Extension and flexion as with the dorsal interossei.
The Lumbrical muscles arise from the tendons of the Flexor digitorum profundus, the two radial usually each by a single head and the two ulnar each by two heads from the sides of adjacent tendons. They insert into the radial side of the dorsal aponeuroses of the second to the fifth fingers. Nerve: The one or two radial by the median, the two or three ulnar by the ulnar. Action: Flex the basal phalanges and extend the terminal ones, the interossei assisting.
The extensor tendons or dorsal aponeuroses, as they may be termed on account of their forming flat expansions on the dorsal surfaces of the digits, include; first, the tendons of the Extensor digitorum communis together with those of the proprii where these occur (index and little fingers), since they fuse with the tendons of the Extensor communis; second, the tendons of the Interossei and Lumbricals which, spreading out fan-like, pass into the expanded tendons of the extensor tendons on the dorsal surfaces of the basal phalanges, but are also continued upon the middle and terminal phalanges. These latter are not reached by the tendons of the Extensor. Consequently, the Extensor extends only the basal phalanges, while the two distal ones are extended by the continued action of the Interossei and Lumbricales.
In the flexor tendons it is to be noted that the tendons of the Flexor digitorum sublimis, which are perforated by the profundus in the region of the basal phalanges, have their insertions in the middle phalanges, while the perforating profundus tendons insert on the terminal phalanges. None of these tendons insert into the basal phalanx, which may be flexed by the action of the Interossei and Lumbricales. Only the small vincula tendinea fasten the tendons of the Flexores digitorum to the volar surfaces of the basal phalanges.
The muscles of the upper extremity fall into four main groups:
The muscles of the upper extremity are enclosed in a common fascia, which receives different names in different regions. At the shoulder there is an axillary fascia, a supraspinatus, an infraspinatus, and a subscapular; on the upper arm the brachial fascia; on the forearm the antebrachial fascia and in the hand the dorsal fascia and the palmar aponeurosis.
The axillary fascia (see also here) is a thin membrane which forms the base of the axillary cavity. It is pierced by many blood vessels and possesses a few stronger deeper bundles extending from the Latissimus to the Pectoralis, these being sometimes muscular and then termed the axillary arch. Anteriorly it becomes directly continuous with the pectoral fascia, posteriorly with the dorsal fascia. The supraspinatus fascia covers the muscle of that name and is partly tendinous in character. The infraspinatus fascia is a very thick, tendinous fascia covering the Infraspinatus and Teres minor and partly also the Teres major, giving origin to some of the fibres of the two former, with which it unites to form an aponeurosis. The rather dense subscapular fascia covers the muscle of that name.
The brachial fascia is continuous above with the fasciae just mentioned and reaches its greatest thickness below the insertion of the Deltoid, but is in general thin and weak. It consists largely of transverse fibres and anteriorly is moulded over the Biceps, on either side of which is a groove, a medial and less noticeable lateral bicipital groove. In the lower part of the upper arm it gives off septa, separating the two muscle groups of that region, a strong and broad medial intermuscular septum extending to the medial epicondyle and a frequently thin lateral intermuscular septum ending at the lateral epicondyle. These septa are attached to the medial and lateral borders of the humerus, respectively, and serve partly for the origin of the muscles which they separate. The medial septum is usually perforated by the ulnar nerve.
The antibrachial fascia is continuous with the brachial in the region of the cubital fossa. Below the elbow joint, especially, it becomes aponeurotic and gives origin to fibres of the proximal portion of the superficial layer of the flexors and extensors of the forearm. The lacertus fibrosus of the Biceps tendon (see here and Fig. A289) is essentially a portion of the fascia, becoming continuous with it. The fascia is weakened in the cubital fossa and over the muscles of the radial group, especially the Brachioradialis and the Extensor carpi radialis, neither of which arise from it. Toward the wrist joint it becomes thickened both dorsally and volarly by bundles of more or less transverse fibres to form the volar carpal ligament (not to be confused with the transverse carpal ligament which is also volar in position) over the flexor tendons and the dorsal carpal ligament, a broad somewhat oblique and very strong fascial band. This latter forms the six tendon compartments for the eight tendon sheaths of the eleven extensor tendons (see Fig. A305), by uniting firmly with the dorsal surfaces of the lower portion of the forearm bones and especially with the ridges on the dorsal surface of the lower end of the radius. In contrast to the brachial fascia the antibrachial has well developed longitudinal fibres, which are especially strong and tendon-like where the fascia becomes aponeurotic and muscle fibres arise from it. This always occurs only in the proximal portion of the forearm (see above) and only rarely extends to its middle portion; in the lowest third of its length, where most of the muscles have become tendons, it does not occur.
The dorsal fascia of the hand passes distally from the dorsal carpal ligament, gradually becoming thinner. In contrast the palmar aponeurosis (see here) is very strong, by far the strongest portion of the entire fascia of the upper extremity.
The muscles of the lower extremity may be classified as those of the rump, those of the thigh, those of the lower leg and those of the foot. The rump muscles pass from the innominate bone to the upper part of the thigh. The muscles of the thigh are arranged in three groups; an anterior extensor group, a posterior flexor and a medial adductor. In the lower leg three groups may again be distinguished: an anterior extensor group, a lateral peroneal group and a posterior flexor group. This last consists of two layers, a superficial and a deep. In the foot are the dorsal extensor and the plantar flexor muscles. The latter may be grouped into the medial muscles, those of the great toe, those of the little toe, the Lumbricals and the Interossei.
The Glutaeus maximus arises from the posterior part of the ala of the ilium behind the posterior gluteal line, from the dorsal surface of the sacrum and from the sacro-tuberous ligament. It is inserted into the gluteal tuberosity of the femur, also sending a slip to the iliotibial band of the fascia lata. Nerve: The inferior gluteal. Action: Extension of the thigh; aids also in adduction and outward rotation.
The Glutaeus medius arises from the lateral surface of the ala of the ilium, above the anterior gluteal line, and is inserted into the lateral surface of the great trochanter. Nerve: The superior gluteal. Action: Abduction of the thigh, assists also by its posterior portion in outward rotation and by its anterior portion in inward rotation.
The Glutaeus minimus arises from the lateral surface of the ala of the ilium, between the anterior and inferior gluteal lines. It inserts into the tip of the great trochanter. Nerve: The superior gluteal. Action: Abduction of the thigh and external and to some extent inward rotation.
The Piriformis arises from the lateral part of the pelvic surface of the sacrum, in the region of the second to the fourth sacral foramina. It passes outward through the great sciatic foramen and is inserted into the tip of the great trochanter. Nerve: Branch from the sciatic or the sciatic plexus. Action: External rotation of the thigh, assists also in abduction.
The Obturator internus arises from the pelvic surface of the circumference of the obturator foramen and from the obturator membrane. It passes out through the lesser sciatic foramen, bends around the base of the ischial tuberosity and inserts into the trochanteric fossa of the femur. The Gemellus superior takes origin from the spine of the ischium and the Gemellus inferior from the ischial tuberosity; they join the tendon of the obturator internus. Nerve: Branches from the sacral plexus. Action: External rotators and adductors.
The Quadratus femoris arises from the lateral border of the ischial tuberosity and passes outwards to the intertrochanteric crest. Nerve: A special branch from the sciatic plexus. Action: External rotation and adduction.
The Tensor fasciae latae arises from the anterior superior spine of the ilium and is inserted into the ilio-tibial band of the fascia lata. Nerve: The superior gluteal. Action: Tenses the fascia lata and assists in flexion and inward rotation of the thigh.
The muscles of the lower limb are enclosed in a fascia, which, in places, is exceptionally strong. That part that covers the Ilio-psoas is termed the iliac fascia, that which invests the muscles of the thigh, the fascia lata, that of the lower leg, the crural, and in the foot there is a dorsal fascia and the strongly tendinous plantar aponeurosis (see here).
The iliac fascia invests the ilio-psoas muscle and, at its medial border, passes over into the pelvic fascia. Below it passes upon the muscles of the thigh and unites with the pectineal fascia to form the ilio-pectineal fascia. This divides the space below the inguinal ligament into two compartments or lacunae, a lateral lacuna musculorum for the Ilio-psoas and the femoral nerve and a medial lacuna vasorum for the femoral vessels.
The fascia lata consists of two layers, separable only in certain areas and varying much in thickness. It is stronger on the posterior and lateral surfaces of the thigh than on the anterior and medial. Its superficial layer, just below the inguinal ligaments, forms a free medial border, the falciform border, which, with the deep layer, the pectineal fascia, forms the boundary of the fossa ovalis. The lower border of the fossa is termed the inferior cornu and the upper the superior cornu. The fossa is closed by a somewhat sieve-like portion of fascia, the fascia cribrosa, a larger opening in this transmitting the great saphenous vein. The fossa represents the external or subcutaneous ring, that is to say, the lower opening of the femoral canal (see here).
On the posterior surface of the thigh the fascia lata covers the Glutaeus maximus by its superficial layer, here quite thin, the deep layer passing beneath the muscle; on the part of the Glutaeus medius that is not covered by the maximus, the fascia forms a dense aponeurotic sheet (fascia glutaea). Some strong transverse fibres run in the gluteal groove at the lower border of the maximus. Over the flexor muscles the fascia lata is of moderate strength and shows predominating transverse fibres, which become especially developed in the region of the popliteal fossa, whose roof is formed by the fascia lata.
The strongest part of the fascia lata occurs on the lateral surface of the thigh; it is the ilio-tibial band (tractus) and is formed mainly of strong tendinous longitudinal bundles of fibres, which are attached below to the lateral condyle of the tibia. Between the groups of thigh muscles the fascia in the lower part of the thigh sends in to the lips of the linea aspera a medial and a lateral intermuscular septum, the medial becoming continuous with the tendon of the Adductor magnus. On the anterior surface of the thigh the fascia is divided in its upper part into two layers; the superficial one covers the surface of the Sartorius and the femoral vessels, the deeper one passes behind the Sartorius, lines the ilio-pectineal fossa and the furrow between the Vastus medialis and the Adductors. Over the Adductors the fascia is thin. The portion covering the Pectineus is termed the pectineal fascia; it unites with the lower end of the iliac fascia to form the ilio-pectineal fascia which lines the floor of the ilio-pectineal fossa.
The crural fascia invests the muscles of the lower leg and covers the muscle-free medial surface of the tibia. It is strongest anteriorly below the knee joint, where it fuses with the extensor and peroneal muscles and with the tendons of the pes anserinus. It sends the anterior intermuscular septum to the anterior crest of the fibula between the Extensors and the Peronaei, and the posterior intermuscular septum to the lateral crest of the fibula, between the Peronaei and the Flexors. On the posterior surface of the lower leg it splits into a superficial and a deep layer, the former covering the Triceps surae, the latter the deep group of Flexors. A special thickening of the crural fascia, in addition to those forming the retinacula (see here), is the transverse crural ligament, which passes transversely between the tibia and fibula above the ankle joint.
The Sartorius arises from the anterior superior spine of the ilium and, crossing the thigh obliquely, inserts into the medial border of the tuberosity of the tibia. It forms with the Adductor longus the femoral trigone (Scarpa's triangle), and covers the adductor canal. At its insertion it forms with the tendons of the Gracilis and Semitendinosus the pes anserinus, beneath which are one or two bursae. Nerve: The femoral. Action: Assists in flexion and abduction of the thigh, flexes the lower leg and rotates it inwards when flexed.
The Rectus femoris arises from the anterior inferior spine of the ilium and the upper margin of the acetabulum. Associated with it and uniting with it in a common tendon are three other muscles. The Vastus medialis arises from the medial lip of the linea aspera and is stronger below than above; the Vastus lateralis arises from the lateral lip of the linea aspera and from the base of the great trochanter, being stronger above than below; and the Vastus intermedius arises from the anterior surface of the femur between the other two, with which it fuses, especially with the medialis: These four muscles constitute what is termed the Quadriceps femoris and unite to form a common tendon, that is inserted into the upper and lateral borders of the patella and, by means of the patellar ligament, into the tuberosity of the tibia. Some of the deep fibres of the intermedius insert into the capsule of the knee joint, forming what is termed the Articularis genu. Nerve: The femoral. Action: Draws the patella upwards, extends the lower leg, and flexes the thigh.
Behind the tendon of the Quadriceps is the supra-patella bursa, which communicates with the knee joint, so that the tendon forms part of the anterior wall of the capsule of that joint. Extensions from the tendon to the fascia of the lower leg form the patellar retinacula. Behind the patellar ligament is a deep infrapatellar bursa.
The Pectineus arises from the pecten of the pubis and is inserted into the pectineal line of the femur. Nerve: The femoral. Action: Adducts the thigh and aids in flexion and external rotation.
The Gracilis arises from the pubis close to the symphysis and is inserted into the medial border of the tuberosity of the tibia. Nerve: The obturator. Action: Adducts the knee when the lower leg is extended, aids in flexion at the knee and rotates the flexed knee inwards.
The Adductor longus arises from the junction of the upper and lower rami of the pubis and is inserted into the middle third of the medial lip of the linea aspera. Nerve: The obturator. Action: Adduction of thigh; assists in flexion and outward rotation: The Adductor brevis arises from the upper ramus of the pubis, nearer to the obturator foramen than the Adductor longus, and is inserted into the upper third of the medial lip of the linea aspera. Nerve: The obturator. Action: Adduction of the thigh; assists in flexion and outward rotation.
The Adductor magnus arises from the lower rami of the pubis and ischium and from the lower border of the ischial tuberosity. The portion arising from the lower ramus of the pubis is sometimes termed the Adductor minimus. The muscle inserts into the medial lip of the linea aspera, from the medial epicondyle to near the gluteal tuberosity. The lower part of the tendon is pierced by the adductor hiatus. Nerve: The obturator and sciatic (tibial). Action: Adducts the thigh, partly assists the glutaeus maximus.
The Obturator externus arises from the outer surface of the circumference of the obturator foramen and from the obturator membrane. It inserts into the trochanteric fossa of the femur. Nerve: The obturator. Action: External rotator of the femur; aids in adduction and flexion.
The Biceps femoris arises by its long head from the tuberosity of the ischium and by its short head from the lower half of the lateral lip of the linea aspera. It is inserted into the head of the fibula. Nerve: The long head by the tibial, the short head by the peroneal. Action: Flexion of the lower leg and extension of the thigh, together with external rotation.
The Semitendinosus arises from the tuberosity of the ischium, with the long head of the Biceps, and is inserted into the medial border of the tuberosity of the tibia, forming part of the pes anserinus. Nerve: The tibial. Action: Flexion of the lower leg, together with internal rotation. Extension and adduction of the thigh.
The Semimembranosus arises from the tuberosity of the ischium and is inserted into the posterior part of the medial condyle of the tibia and into the oblique popliteal ligament. Nerve: The tibial. Action: Flexion and inward rotation of the lower leg; extension and adduction of the thigh.
Where the Glutaeus maximus passes over the great trochanter a trochanteric bursa is interposed and lower down one or several glutaeo-femoral bursae. Under the insertion of the Glutaeus medius there is a bursa, and, similarly, under that of the Glutaeus minimus. Where the Obturator internus tendon passes at an acute angle over the lesser sciatic notch there is an elongated bursa. Between the Ilio-psoas and the ilio-femoral ligament there is an ilio-pectineal bursa that occasionally communicates with the hip joint.
The Gastrocnemius, which has two heads, together with the Soleus forms a muscle mass sometimes termed the Triceps surae. The Gastrocnemius arises by its medial head from the medial condyle of the femur and by its lateral head from the lateral condyle. The two heads unite together and at about the middle of the lower leg the muscle unites with the Soleus lying beneath it. The Soleus takes its origin from the head, posterior surface and lateral crest of the fibula, from a tendinous arch between the tibia and fibula over the popliteal vessels and from the posterior surface of the tibia at and below the popliteal line. The muscle unites with the Gastrocnemius to form a powerful tendon (tendo Achillis) which is inserted into the tuberosity of the calcaneus. Nerve: The tibial. Action: Plantar flexion of the foot; raises the heel.
The Plantaris is a small muscle with a long slender tendon. It arises from the lateral condyle of the femur and is inserted at the heel into the deep layer of the crural fascia and the tendo Achillis. Nerve: Tibial. Action: Tenses the tendo Achillis.
The Popliteus arises from the lateral condyle of the femur and from the arcuate popliteal ligament and is inserted into the posterior surface of the tibia above the popliteal line. Nerve: The tibial. Action: Tenses the capsule of the knee; flexes the knee and rotates it inwards.
A bursa lies beneath the origin of the medial head of the Gastrocnemius and another beneath the origin of the Semimembranosus; both may communicate with the knee joint. A popliteal bursa, beneath the origin of the Popliteus, also communicates with the knee joint.
The Tibialis posterior arises from the upper part of the posterior surface of the tibia, from the interosseous membrane and the medial surface of the fibula. It inserts into the tuberosity of the navicular bone and the plantar surface of the first or all of the cuneiforms. Nerve: The tibial. Action: Plantar flexion and elevation of the inner border of the foot (supination); fixes the head of the talus.
The Flexor digitorum longus arises from the posterior surface and interosseous crest of the tibia. It divides into four tendons which insert into the terminal phalanges of the four lateral toes. Nerve: The tibial. Action: Flexes the terminal phalanges of the four lateral toes, assists in plantar flexion and supination.
The Flexor hallucis longus arises from the posterior surface and the lower two-thirds of the lateral crest of the fibula and from the interosseous membrane. It inserts into the terminal phalanx of the great toe. Nerve: The tibial. Action: Flexes the great toe, acting also on the others (see below), and assists in flexing and supinating the foot. The tendons of the Flexor digitorum longus and Tibialis posterior cross one another above the medial malleolus, so that that of the latter muscle is the more medial at the level of the laciniate ligaments (see Fig. A335). On the sole of the foot there is a crossing of the tendons of the Flexor hallucis longus and Flexor digitorum longus, by which both tendons fuse, so that the strong Flexor hallucis acts not only upon the great toe, but also on the other four.
The Tibialis anterior arises from the lateral surface of the tibia, the interosseous membrane and the crural fascia. It inserts into the medial border of the base of the first metatarsal and into the plantar surface of the medial cuneiform. Nerve: The deep branch of peroneal. Action: Dorsal flexion and supination of the foot; elevation of its inner border.
The Extensor hallucis longus arises from the medial surface of the fibula, the interosseous membrane and the crural fascia. It is inserted into the dorsal surface of the great toe. The Extensor digitorum longus arises from the anterior crest of the fibula, the interosseous membrane and the crural fascia and inserts by four tendons into the dorsal aponeuroses of the four lateral toes. The Peronaeus tertius splits off from the lower part of the Extensor digitorum longus and is inserted into the dorsal surface of the fifth metatarsal. Nerve: The deep branch of the peroneal. Action: Extension of the toes; the Peronaeus tertius assists in dorsal flexion of the foot, the Extensors in supination also.
The Peronaeus longus arises from the head of the fibula, the crural fascia, the upper two-thirds of the lateral surface and lateral crest of the fibula. It passes across the sole of the foot in the peroneal groove and is inserted into the tuberosity of the first metatarsal. The Peronaeus brevis arises from the lower half of the lateral surface and the anterior crest of the fibula and inserts into the tuberosity of the fifth metatarsal, sending prolongations to the fifth toe. Nerve: Both Peronaei are supplied by the superficial branch of the peroneal. Action: raise the lateral border of the foot (pronation) and assist in plantar flexion.
The Extensor digitorum brevis arises from the dorsal and lateral surfaces of the calcaneus, anterior to the sinus tarsi. It passes by three slender tendons into the dorsal aponeurosis of the three middle toes. The Extensor hallucis brevis arises from the dorsal surface of the calcaneus and inserts into the dorsal aponeurosis of the great toe. Nerve: The deep branch of the peroneal. Action: Extensors of the toes.
While the dorsal fascia of the foot is an unimportant thin sheet, the plantar aponeurosis is the strongest of all the fasciae of the leg. At the middle of the sole of the foot it is a thick, tendinous sheet, whose bundles are chiefly longitudinal, but have an oblique direction towards the borders of the foot. The proximal part of the aponeurosis is firmly united to the long plantar muscles and arises with them from the medial and lateral processes of the calcaneal tuberosity; it is much thicker than the distal portion. With this, it presents three plantar eminences, medial, lateral and intermediate. A fibular portion covering the Abductor digiti quinti may be distinguished from the broader tibial portion covering chiefly the Flexor digitorum brevis. From the aponeurosis numerous fine bundles pass to the skin. Towards the toes the tibial part of the aponeurosis divides into several processes, which practically agree in number with the toes, but transverse fasciculi are hardly noticeable, a condition contrasting with that of the palmar aponeurosis where they are very noticeable (see here). In the toes the prolongations of the aponeurosis are lost in the connective tissue of the skin.
The Flexor digitorum brevis arises from the medial process of the calcaneal tuberosity and from the plantar aponeurosis. It inserts by four tendons, which are perforated by the tendons of the long flexor, into the middle phalanges of the four lateral toes. Nerve: The medial plantar. Action: Flexes the toes.
The Quadratus plantae arises by two heads from the plantar surface of the calcaneus and from the long plantar ligament. It is inserted into the tendon of the Flexor digitorum longus. Nerve: The lateral plantar; Action: Assists the flexor digitorum longus, correcting its oblique pull.
The Abductor hallucis arises from the medial process of the calcaneal tuberosity and from the plantar aponeurosis. It inserts by means of the medial sesamoid bone into the basal phalanx of the great toe. The Flexor brevis hallucis arises from the plantar surfaces of the second and third cuneiforms and from the long plantar ligament. It is inserted by two heads into two sesamoid bones and the basal phalanx of the great toe. The Adductor hallucis consists of two distinct portions. The oblique head arises from the plantar surface of the third (lateral) cuneiform and the plantar ligament. The transverse head arises from the tarso-metatarsal joints of the fifth to the third toe. It is inserted into the lateral sesamoid bone and basal phalanx of the great toe. Nerves: For the Abductor and Flexor brevis the medial plantar; for the Adductor and part of the Flexor the lateral plantar. Action: Adduction and flexion of the great toe.
The Abductor digiti quinti arises from the lateral process of the tuberosity of the calcaneus and from the plantar aponeurosis, further, by a deep head, from the medial process of the calcaneal tuberosity. It inserts into the lateral border of the basal phalanx of the little toe and into the tuberosity of the fifth metatarsal. The Flexor digiti quinti brevis and the Opponens digiti quinti arise in common from the anterior part of the long plantar ligament. The Flexor inserts into the basal phalanx of the little toe, the Opponens into the lateral border of the fifth metatarsal. Nerve: The lateral plantar. Action: Abduction, flexion and opposition of little toe.
The Lumbricals of the foot arise from the tendons of the Flexor digitorum longus, the first by a single head from the medial edge of the first (medial) tendon, the other three by two heads. In the region of the metatarso-phalangeal joint they pass to the medial side of the dorsal aponeurosis of the four lateral toes. At their points of insertion there are usually small bursae. Nerves: They are supplied in a variable manner by the medial and lateral plantars. Action: Flexion of the basal phalanges and extension of the others.
The Interossei (see Fig. A336 and A337) are seven in number, four Dorsal and three Plantar. They occupy the inter-metatarsal spaces and the plantar arise by single heads, the dorsal by two. The first dorsal inserts into the dorsal aponeurosis of the second toe on the tibial side, the other three into the fibular side of the aponeurosis of the second, third and fourth toes. The plantar insert into the tibial side of the aponeurosis of the third, fourth and fifth toes. Nerve: The lateral plantar. Action: Flexion of basal phalanges, extension of the others.
The dorsal aponeurosis of the toes are essentially like those of the fingers. They are formed by the tendons of the Extensor brevis and Extensor longus, those of the Interossei and those of the Lumbricales.
The three groups of muscles passing from the lower leg into the foot have their tendons invested by tendon sheaths, which, like those of the upper extremity, are protected by retinacula. For the two Peronaei there is a double retinaculum, which is actually a thickening of the deep layer of the lateral portion of the crural fascia. The superior peroneal retinaculum extends from the neighborhood of the lateral malleolus to the calcaneus, the inferior peroneal retinaculum from the neighborhood of the trochlear process of the calcaneus, above which it blends with the cruciate ligament, to the lateral border of the plantar surface of the bone. If the trochlear process is well developed it separates the tendons and tendon sheaths of the two Peronaei. While the sheath of the Peronaeus brevis tendon ends a little beyond the process that of the longus extends into the sole of the foot, where it receives a new retinaculum, formed by the anterior part of the long plantar ligament (see here).
At the medial malleolus the retinaculum for the flexor muscles, the Tibialis posterior, Flexor digitorum longus and Flexor hallucis longus, is formed by the broad laciniate ligament, which is indistinctly separated from the crural fascia.
On the dorsum of the foot the cruciate ligament is a forked strengthening of the dorsal fascia of the foot, which forms the retinaculum for the Extensor tendons. It consists of a usually strong transverse portion (see Fig. A328), which passes from the medial malleolus to above the trochlear process of the calcaneus, and a band, at right angles to the transverse one, extending from the dorsal surface of the navicular to the anterior part of the calcaneus. The ligament contains three compartments for the tendons of the Tibialis anticus, the Extensor hallucis longus and the Extensor digitorum longus plus the Peronaeus tertius.
The body can be divided into a number of regions that are shown on Fig. A338, A339, A340, A341 and A342.
The mouth cavity (cavum oris), the beginning of the entire digestive tract, is an irregularly shaped, longish cavity in the lower part of the face, and has partly bony, and partly muscular walls. It is divided imperfectly into two portions by the teeth, the oral vestibule and the mouth cavity proper.
The vestibule is a small, somewhat semicircular space, between the lips and cheeks on the one side and the teeth on the other. When the teeth are in contact, it communicates behind the last molar with the actual mouth cavity and in front through the mouth cleft (rima oris) with the outer world. The two lips (labia) form the greatest part of the anterior wall of the vestibule and unite at the angles of the mouth in the labial commissures. The upper lip is somewhat longer than the lower one and on its outer surface presents a flat, rather broad, median furrow, the philtrum. An oblique, slightly arched groove, the nasolabial groove, passes from the ala of the nose toward the cheek. On the outer surface of the lower lip the mento-labial groove separates the lip from the chin (mentum). The lips consist of the skin with hairs, the Orbicularis oris muscle and mucous membrane. This last contains the labial glands, which are mucous glands of small size. The posterior surfaces of the lips in the middle line are connected with the mucous membrane, gingiva, covering the alveolar process of the maxilla and mandible, by thin folds of mucous membrane, the frenula, that of the upper lip being usually the larger and more distinct.
Lateral to the lips the cheeks (buccae) form the wall of the oral cavity. Like the lips they consist of the skin, with stronger hairs in the male, of the Bucinator muscle and of mucous membrane. The last is thin in this region and contains the buccal glands, which are embedded in the Bucinator muscle or even lie on its outer surface. In the angle between the Bucinator and the Masseter there is a strong development of fat tissue, the buccal fat pad (corpus adiposum buccae) which extends in the new-born child over the whole region of the cheek.
The mouth cavity proper is bounded above by the palate, which separates it from the nasal cavity. The floor of the mouth is formed principally by the tongue, which, when the mouth is closed, fills the cavity, except for a relatively small cleft between its dorsal surface and the palate. The anterior and lateral boundaries are formed by the dental arches, the posterior partly by the soft palate and the palatine arches (pillars of the fauces) and, further, at its posterior wall, it communicates with the oral portion of the pharynx by the isthmus of the fauces.
The palate consists of two portions, the hard palate and the soft palate. The former repeats the form of the palatal plates of the skeleton; its mucous membrane is thick and firm, connected closely by submucous bundles of fibres to the periosteum of the bones. It contains numerous mucous glands. In the median line the mucous membrane is raised into a low ridge, the raphe, and at the anterior end of this, at a point corresponding to the incisive foramen, there is an elongated, wart-like elevation, the incisive papilla, and anteriorly on either side three or four transverse palatine folds, which often disappear in old age, but may be in greater number in the new-born child.
The soft palate is a soft plate separating the mouth cavity from the nasal portion of the pharynx. It is muscular, is abundantly supplied with glands and is covered by mucous membrane on both surfaces. It is attached by its base to the posterior border of the bony palate, its mucous membrane passing directly into that of the palate, and it hangs obliquely downwards and backwards and ends in a rounded conical process, the uvula. This, when the palatal muscles are at rest, lies in such a position that its tip is directed forwards. The mucous membrane of the soft palate is rather smooth, much thinner than that of the hard palate, and is usually well supplied with glands. The lateral parts of the soft palate, the palatine arches (pillars of the fauces) are folds of mucous membrane containing muscles; they bound the isthmus of the fauces i.e. the transition from the mouth cavity to that of the pharynx (see here).
The teeth (dentes) are conical structures imbedded by their roots (radices) in the alveoli of the jaws. The part surrounded by the gingiva is termed the neck (collum), the part projecting into the mouth cavity the crown (corona). Of the three principal constituents of the teeth, the enamel, dentine and cement, the enamel occurs only on the crown, the cement only on the root; at the neck the enamel and cement meet. The enamel has a shining surface and is white with a bluish or yellowish tinge, while the cement is pale yellow and dull. On each crown there is a masticatory surface turned toward the teeth of the upper jaw; the surface turned towards the lips or cheek is the labial or buccal surface; that turned towards the tongue the lingual surface; and those in contact with adjacent teeth the contact surfaces.
The root of a tooth is simple or multiple and is in general conical in shape. It bears at its apex a foramen that leads into a root canal, which traverses the whole length of the root and at the level of the neck broadens to a large cavity, the pulp cavity (cavum dentis), in the interior of the crown, filled with a soft tissue, the pulp. The pulp cavity has in general the form of the tooth, but possesses, almost regularly, fine processes corresponding to the relief of the crown. The tips of the canines are slightly worn. The root canal is also a part of the tooth cavity and accordingly also contains pulp.
The dentition of an adult consists of thirty-two teeth which are arranged in an upper and lower row, the upper and lower dental arches. The upper teeth are implanted in the alveoli of the maxillae, the lower in those of the mandible. The teeth of the two rows resemble each other in form and size, without being exactly alike. The number in each row is sixteen.
The teeth of both jaws may be divided according to their form into four groups, the incisors, canines, praemolars and molars. In each half of each row there are two incisors, one canine, two praemolars and three molars. The teeth of each group represent a well-defined type, without transitions to the others, but within each type there are individual differences, as, for instance, between the corresponding teeth of the upper and lower jaws. The incisors are the most anterior, those of the two sides being in contact in the median line; then follows the canine, then the praemolars, the molars being the most posterior. The human dental formula is as follows:

The incisors have chisel-shaped crowns, convex on the labial and concave on the lingual side; they are thicker but narrower at the base, but become broader and thinner towards their free edge. The labial surface has frequently three indistinct longitudinal ridges separated by furrows. Their crowns are in the frontal plane, so that their contact surfaces are medial and lateral. On account of their chisel-shaped crowns they have no masticatory surface, but a cutting edge, originally three-lobed. The medial angle of this edge is sharp, the lateral rounded. At the base of the crown immediately above the neck there is a thickening, the tubercle. The roots are round, of moderate length and usually almost straight, those of the lateral incisors are usually shorter and slightly flattened. The upper ones are usually larger than the lower and the upper medial is always larger than the lateral, while in the lower jaw the lateral is the larger (Length up to 24 mm).
The canines have a long conical form. Their large and thick crown is conical and stands almost in the frontal plane, so that they present labial and lingual surfaces and medial and lateral contact surfaces, Their rounded tips are not exactly in the axis of the tooth, but slightly to the medial side, the labial surface is strongly convex and the lingual is provided with a tubercle. The root is very long and also conical, yet, especially in the lower ones, distinctly flattened. The canines, especially the upper ones, are the longest teeth in the dentition (on account of their long roots - 35 mm).
The praemolars possess bitubercular (bicuspid) crowns, flattened from before backwards; their contact surfaces are anterior and posterior and their lingual and buccal surfaces convex. The two tubercles are separated by an almost sagittal furrow that follows the curve of the dental arch, so that there is a weaker lingual and a stronger buccal tubercle. The lingual tubercle of the first lower praemolar is usually feebly developed and the lingual of the second lower (also low) is often double, so that this tooth may be tritubercular. The roots of the lower praemolars are always simple, of moderate length and distinctly flattened; those of the upper sets vary greatly, that of the first being usually double or at least cleft, that of the second only strongly flattened or furrowed. One root is buccal, the other lingual. The first upper praemolar is larger than the second.
The molars all possess large, low crowns with several tubercles and have two or three roots, these, as well as the positions of the tubercles differing in the upper and lower teeth. The upper molars have three roots, the larger, lower ones only two. The first molar in both the upper and lower sets has the largest and highest crown, the third the smallest and lowest. The tubercles are four, rarely five in number, two being on the lingual and two on the buccal side. In the lower molars a rather regular crucial furrow separates the four tubercles, of which the lingual are higher than the buccal. The first lower molar has usually five tubercles, three buccal and two lingual. In the upper molars the buccal tubercles are higher than the lingual and the intervening furrow has the form of an oblique H, so that the lingual and buccal tubercles are not exactly opposite one another. Frequently, but not always, the first upper molar has a super-numerary tubercle, usually very small, at the base of the anterior lingual tubercle. It is the so-called anomalous (Carabelli) tubercle. The contact surfaces of the molars are anterior and posterior.
The lower molars have two conical roots, an anterior (somewhat the stronger) and a posterior; they are flattened in the frontal plane, are furrowed and of considerable size, and their tips are usually curved backwards. The upper molars, on the contrary, have three conical roots, two buccal and one lingual or palatal; their tips are also curved. All three roots are usually well developed in the first upper molar; in the second they show, not infrequently, more or less fusion, and this is the rule in the third upper one in which the roots are almost parallel. In the upper molars the tips of the roots are often slightly curved backwards.
The third molars, also called wisdom teeth (dentes serotini), are usually more or less rudimentary. The upper is always much smaller than the lower and its roots usually fuse to a single mass with indications, in three root canals, of their original triple division. Often they possess only three tubercles, sometimes more than four. The lower wisdom tooth has usually two short roots and a crown that departs somewhat from the type.
The permanent dentition of the adult, consisting of thirty-two teeth, is preceded in childhood by a Milk dentition of only twenty teeth (dentes decidui) including eight incisors, four canines and eight molars. The formula for the milk dentition is therefore:
The incisors and canines of the milk dentition resemble the corresponding teeth of the permanent dentition not only in general but also in particular, though they are relatively smaller and the furrows are wanting on the labial surfaces of the crowns of the incisors. These teeth also occur in the same position as their successors, while the milk molars appear in the places later occupied by the praemolars. The milk molars, while resembling the permanent ones, represent a specific type; they have more than one root and have several tubercles. The second (posterior) are larger than the first; the upper ones have usually three roots like the permanent molars, two buccal and one lingual, while the lower have two roots. The crowns have three (anterior) to five (posterior) irregularly placed tubercles, which are separated by very irregular furrows.
The first milk tooth to erupt, on the average, in the sixth or seventh month after birth, is the medial incisor of the lower jaw, the teeth of the lower jaw as a rule appearing earlier than those of the upper. Then, in the seventh or eighth month the corresponding tooth of the upper jaw appears. The lateral incisors erupt usually from the eighth to the twelfth month; the anterior molars of the lower jaw from the twelfth to the sixteenth month; those of the upper jaw some months later; after these the canines, from the sixteenth to the twentieth month; and, finally, the posterior molars from the twentieth to the thirtieth month.
The milk dentition is gradually replaced by the permanent teeth, so that for a time representatives of both dentitions are present. The first, lower, permanent molars erupt at the fifth to the eighth year and soon after the corresponding teeth of the upper jaw appear. Later the process of replacement begins and, in the sixth to the ninth year, the median milk incisors are replaced by the permanent ones, and then the lateral ones in the seventh to the tenth year. The first praemolars erupt in the ninth to the thirteenth year; the permanent canines in the ninth to the fourteenth; the second praemolars in the tenth to the fourteenth; Replacement now ends and soon after, in the tenth to the fourteenth year, the second molars appear; the third molars erupt much later, in the sixteenth to the fortieth year or not at all. The upper praemolars usually appear before the lower, but otherwise the lower teeth precede the corresponding upper ones.
The tongue (lingua) presents for examination three parts, a body (corpus), the largest, middle portion, adherent to the floor of the mouth, an apex projecting freely into the mouth cavity anteriorly and a root (radix) posteriorly, attached to the hyoid bone and the epiglottis.
The inferior surface of the body is attached; the convex upper surface, lined throughout its whole extent by the oral mucous membrane, is termed the dorsum. The entire surface of the tongue facing the palate is also termed the dorsum linguae. The lateral border is free in the anterior part of the tongue, but behind passes into the soft palate by means of the glossopalatine arch. The boundary between the body and the root is indicated on the dorsum by the foramen caecum, which leads into a quite short, blindly ending canal, the lingual (thyreoglossal) duct. The vallate papillae extend outward and forward from the foramen caecum, forming an angle open anteriorly and with its apex at the foramen (V-shaped). Frequently, immediately behind and parallel to the vallate papillae there is a groove, the terminal sulcus, which, when present, marks the boundary between the body and the root. The root is connected with the epiglottis by three folds of mucous membrane, a median glosso-epiglottic fold and two lateral glosso-epiglottic folds. Between these there is on either side a roundish depression, the epiglottic vallecula.
The tongue is composed of two principal constituents, the mucous membrane and muscles. The mucous membrane of the dorsum is intimately connected with the subjacent muscle tissue, that of the under surface is only loosely connected with it. The mucous membrane of the under surface is smooth and thin and in the median line below the apex forms a sagittal fold, the frenulum. On either side of this there is a low fold with lobed edges, the plica fimbriata, which is well developed in the new-born child, but often less distinct in the adult. It runs from the anterior end of the frenulum posteriorly and laterally. At the margins of the tongue another fold of mucous membrane, the sublingual fold, runs obliquely anteriorly and median ward, to terminate at the root of the frenulum in a sublingual caruncle; it corresponds to the submaxillary duct (see here) which lies close beneath the mucous membrane. The mucous membrane of the dorsum of the tongue is divided by the terminal sulcus or vallate papillae into that of the body and tip, the papillary portion, and that of the root, the tonsillar portion.
The papillae of the mucous membrane of the anterior part of the tongue are in general conical; they project above the surface of the mucous membrane and give it a satiny appearance. They are divided by their form into:
Quite different from the anterior, papillary portion of the lingual mucous membrane is the posterior tonsillar portion, characterized by the occurrence in it of lymphatic lingual follicles, which in their sum total form the diffuse lingual tonsil. Each follicle is a small round elevation 2-3 mm in diameter, with a central, fine depression. As a whole they form on the actual root of the tongue a closely packed, almost defined mass, while towards the epiglottis and the neighbouring palatine tonsils they are more scattered.
The muscles of the tongue consist of two groups:
The Genio-glossus arises from the internal mental spine and passes mainly to the under surface of the mucous membrane of the dorsum of the tongue and partly also to the hyoid bone and the epiglottis.
The Hyoglossus and Chondro-glossus arise from the body and greater cornu of the hyoid bone (the Chondro-glossus from the lesser horn). They pass anteriorly and upwards to the lateral portions of the tongue, interlacing with the fibres of the second group.
The Stylo-glossus arises from the styloid process of the temporal bone and passes to the border of the tongue, interlacing with the fibres of Group II.
The Longitudinalis inferior lies on the under surface of the tongue between the Genio-glossus and Hyoglossus and extends from the root to the tip; it is almost cylindrical. The Longitudinalis superior consists of longitudinal fibres situated at the dorsum of the tongue; they are really fibres of the Hyoglossus and Styloglossus. The Transversus linguae is composed of transverse fibres that pass from the septum of the tongue to the lateral surfaces; in front of the anterior end of the septum they pass from side to side, posteriorly they pass over into the Glosso-palatinus and Glosso-pharyngeus. The Verticalis linguae is formed by muscle bundles passing from the dorsum to the under surface of the tongue.
All the above muscles are supplied by the hypoglossal nerve.
The musculature of the tongue is incompletely divided into two halves by the septum of the tongue, a sheet of somewhat fatty connective tissue which does not quite reach the dorsum linguae.
Fig. B39 shows the topographic relations of the mouth cavity, cavum oris. The upper and lower dental arcades in the position of occlusion form the boundaries of both portions of the mouth cavity, the vestibulum oris and the cavum oris proprium; the former is bounded anteriorly by the lips.
When the mouth is closed the mouth cavity proper is practically filled by the tongue; it is separated from the nasal cavity by the hard palate, palatum durum, and from the upper or nasal portion of the pharynx by the soft palate, palatum molle or velum palatinum. The floor of the cavity is formed by the anterior and middle portions of the dorsum of the tongue, for only these portions of the tongue's surface look upward. Its posterior portion, the so-called radix linguae, looks almost backward when the mouth is closed and lies opposite the anterior wall of the pharynx in the region of the isthmus faucium, the wide opening of communication between the oral and pharyngeal cavities. Beneath the tongue are the muscles of the floor of the mouth, the Mylohyoid and the Geniohyoid, extending from the mandible to the hyoid bone. The root of the tongue passes over into the anterior (oral) surface of the epiglottis in front of which is a fat body.
The lower portion of the pharynx behind the larynx is a cleft, very narrow in the median line, and passes without any demarcation into the oesophagus. In its upper part, close under the epiglottis is the entrance into the larynx, aditus laryngis. Just as the transition of the pharynx into the oesophagus is shown, So too is that of the larynx into the trachea. Further, one may perceive the apposition of the posterior wall of the pharynx to the anterior surfaces of the cervical vertebrae and their intervertebral fibrocartilages and that of the roof of the pharynx to the base of the skull.
The figure also shows how the action of the muscles of the soft palate brings its free border into contact with the anterior surface of the posterior wall of the pharynx and so produces a closure of the upper portion of the pharynx from the middle portion, such as is brought about in swallowing and also in speaking (except for the nasal sounds).
There are two groups of glands that take part in the formation of the saliva: the numerous small glands in the walls of the mouth cavity and the three pairs of large salivary glands, the parotid, the submaxillary and the sublingual which lie outside the boundaries of the mouth cavity. The last form a transition to those of the first group.
The parotid glands are the largest of the salivary glands. They are flattened, almost triangular, but of somewhat irregular form, and are situated one on either side in front of the ear and in the immediately adjacent parts of the neck. The slightly convex, almost smooth, lateral surface is covered by the skin of the cheek, by offsets from the Platysma and by the parotideo-masseteric fascia, while its slightly concave medial surface rests principally on the Masseter (partly also on the ramus of the mandible), from which it is separated by a thin layer of deep fascia. The anterior, slightly concave border lies throughout its entire length on the outer surface of the Masseter. This portion is much thinner than the more posterior portion, which constitutes the main mass of the gland. It extends into the neck along the anterior border of the Sternocleidomastoideus to the retromandibular fossa and even into the submaxillary region. A process of the gland, the retromandibular process, extends beneath the ramus of the mandible to the posterior belly of the Digastricus and to the muscles arising from the styloid process, surrounding as a compact mass of glandular tissue the external auditory meatus; this portion constitutes the main mass of the entire gland (see Fig. B107). The distinctly lobed, reddish brown gland is abundantly traversed by nerves and blood-vessels, chiefly by the branches of the facial nerve.
The parotid duct (Stenson's) arises above the middle of the anterior border of the gland and runs almost horizontally forward over the Masseter and, shortly before reaching its anterior margin, bends medially to pass through the buccal fat pad and the Bucinator muscle to reach the mucous membrane of the mouth. It is a somewhat flattened, rather thick-walled duct about the size of a crow-quill; its oval, slit-like orifice opens into the vestibule of the mouth opposite the second upper molar tooth. Very frequently an accessory parotid, resembling the main gland, but very variable in size, occurs on the parotid duct.
The submaxillary gland is an oval, slightly flattened structure, about the size of a plum. It lies in the neck, in the submaxillary region, immediately beneath the Platysma and the superficial cervical fascia. It lies mainly below the mylohyoid muscle, which separates it from the sublingual gland, and fills the space between the angle of the mandible and the two bellies of the Digastricus, bordering also on the Stylo-hyoid, Stylo-glossus and partly the Hyo-glossus. It is more coarsely lobed than the parotid and is paler in color. Its upper part forms the submaxillary fovea on the mandible (see Fig. A99 and A100), while its main mass is below the base of that bone.
A thin, strongly flattened process of the gland extends upwards between the Internal pterygoid and Mylohyoid and anteriorly to the sublingual gland. The thin walled submaxillary duct (Wharton's), about the size of a small quill, passes from the upper part of the gland above the Mylohyoid, between that muscle and the mucous membrane of the floor of the mouth, and runs forward and medially, medial to the sublingual gland, producing the sublingual fold, to the sublingual caruncule beside the frenulum of the tongue. The external maxillary (facial) artery lies in a deep groove on the upper medial surface of the gland.
The sublingual gland lies immediately below the mucous membrane of the floor of the mouth and is an elongated, strongly flattened structure. It is placed almost sagittally and is visible through the mucous membrane, lateral to the sublingual fold, if the tip of the tongue is raised. Its lateral border lies in the sublingual fovea of the mandible, its posterior part borders upon the submaxillary gland, and its medial border upon the Genio-glossus; its under surface rests upon the Mylohyoid. It is the smallest of the three salivary glands and is but slightly compact, being usually composed of several portions only loosely connected (see here).
One may indeed recognize an anterior monostomatic, greater sublingual gland and a posterior polystomatic complex of glands, the lesser sublingual gland. The former has a single duct about the thickness of a small quill, by means of which it pours its secretion into the mouth cavity at the sublingual caruncula. The lesser gland is sometimes not sharply separated from the greater and has six to twelve ducts, which open by minute openings on the anterior part of the sublingual fold. Loose connective tissue binds the two portions into an apparently single mass.
The smaller glands of the mouth cavity are:
All these glands fall far short of the size of the three large salivary glands. The majority are about the size of a hemp seed.
The pharynx is an unpaired cylindrical tube, slightly flattened from before backwards and placed vertically. It is completely closed laterally and posteriorly by muscular walls and anteriorly is in open communication with the nasal and mouth cavities and, below, with the larynx. Its roof is formed by the base of the skull. The posterior wall is in contact behind with the anterior surfaces of the cervical vertebrae and it extends to a level between the sixth and seventh of these vertebrae, where it passes into the oesophagus. Like the lateral walls the posterior is formed principally by the constrictor muscles; the anterior wall has no special muscles. The Stylopharyngeus muscle serves to suspend it to the base of the skull.
The Superior constrictor of the pharynx (Cephalo-pharyngeus) may be regarded as composed of four parts. The Pterygo-pharyngeus arises from the hamulus of the sphenoid; the Bucco-pharyngeus from the pterygo-mandibular raphe; the Mylopharyngeus from the mylo-hyoid line of the mandible; and the, Glosso-pharyngeus from the transverse fibres of the tongue. These parts unite and interlace in the pharyngeal raphe.
The Middle constrictor (Hyo-pharyngeus) has two portions. The Cerato-pharyngeus arises from the greater cornu of the hyoid, the Chondro-pharyngeus from the lesser cornu. They unite to pass to the pharyngeal raphe.
The Inferior constrictor (Laryngo-pharyngeus) has also two parts. The Thyreo-pharyngeus arises from the oblique line of the thyreoid cartilage and the Cricopharyngeus from the lateral border of the cricoid cartilage. These, too, insert into the pharyngeal raphe.
The Stylo-pharyngeus arises from the styloid process of the temporal and is inserted into the wall of the pharynx between the Middle and Superior constrictors.
The upper border of the Superior constrictor is two cm below the base of the skull, so that in the uppermost part of the posterior and lateral walls of the pharynx the fibrous coat, with the pharyngeal glands, forms the outer wall of the cavity (Fig. B45).
The constrictor muscles of the two sides unite behind in a median pharyngeal raphe. They are not simply in contact with one another, but, especially in their lower part, overlap to a greater or less extent. For this reason in a view of the pharyngeal wall from behind it seems to be formed over far the greatest part by the largest of the three constrictors, the Constrictor inferior, this partly overlapping the Constrictor medius from below, just as this overlaps the Constrictor superior. Since the muscles broaden posteriorly this arrangement is more evident from behind (Fig. B45) than in a lateral view (Fig. B46).
The Stylopharyngeus sinks into the pharynx wall between the Superior and Middle constrictors. Occasionally a small muscle slip passes to the Superior Constrictor from the base of the skull.
The posterior wall of the pharynx in the median line lies on the anterior surfaces of the cervical vertebrae, laterally on the anterior surface of the praevertebral muscles of the neck, from which it is separated by the praevertebral fascia.
The Constrictors are supplied by the vagus and glosso-pharyngeal nerves through the pharyngeal plexus; the Stylo-pharyngeus by a branch from the glosso-pharyngeal.
These muscles lie partly in the soft palate and serve for its movement (closing off the nasal from the oral portion of the pharynx) as well as for the opening of the cleft-like lumen of the tuba auditiva (Eustachian tube). They are also partly muscles of the isthmus of the fauces, which they may contract. Both groups spread out in the muscular wall of the pharynx.
The musculus (azygos) uvulae, usually unpaired, arises from the posterior nasal spine and passes to the uvula.
The Levator veli palatini arises from the lower surface of the petrous portion of the temporal and from the cartilage of the tuba auditiva (Eustachian tube). The muscles of either side interlace in the soft palate.
The Tensor veli palatini arises from the angular spine and scaphoid fossa of the sphenoid and from the lateral surface of the cartilage of the tuba auditiva. Its flat tendon passes over the hamular groove and expands to form with the muscle of the other side a membranous sheet, the palatine aponeurosis, in the substance of the soft palate.
The Glosso-palatinus (Palato-glossus) is formed from the transverse fibres of the tongue. It passes down in the arch of the same name to the soft palate.
The Pharyngo-palatinus (Palato-pharyngeus) is formed from the middle and inferior constrictors of the pharynx. It passes upward in the arch of the same name to the soft palate.
The musculus uvulae, Levator, Glosso-palatinus and Pharyngo-palatinus are supplied by branches of the vagus and glosso-pharyngeal nerves, through the pharyngeal plexus. The Tensor is supplied by a branch from the mandibular division of the trigeminus that passes through the otic ganglion.
The cavity of the pharynx consists of three portions, one situated above the other and not distinctly separated from one another, the nasal, oral and laryngeal portions. The nasal portion communicates with the nasal cavity through the choanae and is separated from the mouth cavity by the soft palate. Its roof, which lies immediately beneath the base of the skull is termed its fornix. On either side, on its lateral wall opposite the opening of the inferior meatus of the nose at the choanae, is an oval opening, the pharyngeal opening of the tuba auditiva (Eustachian tube). The lips of the opening are anterior and posterior; the anterior is the larger and contains the free end of the cartilage of the tuba auditiva, which projects as a rounded swelling, the torus tubarius (see Fig. B49 and B50). Above and behind the torus there is on either side in the fornix of the pharynx a deep, blind sack, the pharyngeal recess (Rosenmüller's). Between the openings of the two tubae is an unpaired pharyngeal tonsil, which usually becomes rudimentary in the adult. Anterior and medial to the opening of the tuba an elevation of the mucous membrane, the levator swelling, passes obliquely downward to the soft palate (Fig. B49). The anterior lip of the tubal opening is continued downward towards the posterior border of the hard palate as the salpingo-palatine fold, while the salpingo-pharyngeal fold extends downwards from the torus tubarius and sometimes contains a muscle of the same name.
The oral portion of the pharynx is in direct continuity with the mouth cavity through the isthmus of the fauces and is separated from it by the pharyngo-palatine arches. It is the narrowest part of the pharynx, but otherwise presents no marked peculiarities.
The laryngeal portion is separated from the oral portion by a fold, the pharyngo-epiglottic fold, which passes to the epiglottis from the lateral wall of the pharynx. The laryngeal is the only portion which has a distinct anterior wall. It lies behind the larynx, whose posterior surface is so closely associated with the mucous membrane of the pharynx that the latter shows a median elevation, corresponding to the cricoid and the arytenoid cartilages, and two lateral, deep depressions, the piriform recesses. In these on either side there is generally an oblique elevation, passing from above downwards and medially, the fold for the laryngeal nerve: Furthermore, the opening (aditus) of the larynx lies in the upper part of this portion of the pharynx.
The wall of the pharynx consists of a mucous membrane, a fibrous coat and a muscular coat. The reddish, rather smooth and thin mucous membrane contains in its upper part small mucous pharyngeal glands. The fibrous coat in the uppermost part of the pharyngeal wall, where the muscular coat is lacking for an extent of about two cm., forms a strong membrane, the pharyngo-basilar fascia, which is attached above to the skull. The muscular coat occurs upon the lateral and posterior surfaces, except in their uppermost parts; it consists essentially of circular fibres, the Constrictors of the pharynx (see Fig. B45, B46), which unite and partly interlace posteriorly in a median raphe (see here).
In addition there are other muscles in the pharyngeal wall, which at the same time belong to the soft palate, since the posterior surface of this forms at the same time the anterior wall of the nasal portion of the pharynx (Fig. B47).
The anterior glosso-palatine arch runs from the lateral, lower border of the soft palate to the mucous membrane of the border of the tongue, where it ends as the triangular fold. The posterior pharyngo-palatine arch is thicker than the anterior, but less strongly arched; it passes from the soft palate to the lateral wall of the oral portion of the pharynx. Between these two arches is a niche, the sinus tonsillaris, in which is situated the palatine tonsil. This is an oval elevation, usually without clearly defined boundaries but with deep clefts and fossae on its surface. It frequently does not completely fill the space between the two palatine arches, a deep depression, the supratonsillar fossa, lying above it. It is often continuous with the neighbouring lingual tonsil (see here), completing the lymphatic pharyngeal ring.
The oesophagus is a muscular tube, about 25 cm in length, which when empty has a flattened cylindrical form. It is the continuation downward of the lower part of the pharynx and passes to the cardiac portion of the stomach. It may be divided into cervical, thoracic and abdominal parts. The cervical part lies at first behind the larynx and immediately in front of the cervical vertebrae, but quickly shows a slight inclination to the left, so that its lower portion is distinctly to the left of the trachea. The thoracic part, by far the longest part, lies at first in the superior mediastinum in front of the bodies of the thoracic vertebrae and almost in the median line, but at the bifurcation of the trachea it lies more under the origin of the left bronchus. Below this the oesophagus enters the posterior mediastinum and is in relation to the posterior wall of the pericardium and the descending aorta, which lies to the left of it, both being for a short distance almost parallel. Gradually, however, the oesophagus passes more and more to the left and in front of the aorta, which thus separates it from the bodies of the vertebrae, and later it passes very obliquely across the front of the aorta and comes to lie to the left of the median line. In general it may be said that the course of the oesophagus is practically in the median line until shortly before its passage through the Diaphragm.
The abdominal part is only about 1 cm in length. In passing the oesophageal opening of the Diaphragm, the oesophagus rather suddenly inclines to the left and opens into the stomach at the level of the eleventh thoracic vertebra. The caliber of the oesophagus is not constant throughout its length, narrower and wider portions alternating with one another. The narrowest parts are:
In the empty state the variations in caliber are hardly noticeable.
The walls of the oesophagus consist of three layers:
The outer and inner coats are completely separated by the intervening looser submucosa. The outer longitudinal muscle layer produces a distinctly striated appearance in the outer surface of the organ, except above where circular fibres predominate.
Except in the abdominal part, which receives a serous investment from the peritoneum, the oesophagus is imbedded in loose adventitious connective-tissue. From the muscular coat bundles occasionally pass to the mediastinal pleura that invests the oesophagus (m. pleuro-oesophageus), and to the posterior wall of the left bronchus (m. broncho-oesophageus).
The stomach (ventriculus) is a sack-like, pear-shaped enlargement of the digestive tract, interposed between the oesophagus and the intestine. The region where the oesophagus opens into it is termed the cardia, the passage to the intestine on the right is the pylorus. In the empty stomach an anterior and a posterior wall may be distinguished, both being convex and separated by the borders or curvatures of the stomach. Of these the greater curvature is almost three times as long as the lesser curvature; the former looks upwards, laterally and downwards and is throughout convex, the lesser curvature, on the other hand, is concave (except in the pyloric region) and looks medially (upwards in the pyloric region). At the lesser curvature the peritoneum is attached to the stomach as the lesser omentum and at the greater curvature it leaves it as the greater omentum. Three principal portions may be distinguished in the stomach, a fundus, a body (corpus) and a pyloric portion; the cavity of the last is termed the pyloric antrum, or, better, the pyloric canal.
The body is the principal portion of the stomach and, especially in the living, has an almost vertical position (in the atonic condition in the cadaver it is more or less transverse); in it is the lowest point of the stomach (also termed the sinus). That portion of the stomach that is uppermost and to the left is the fundus; it is in contact with the left dome of the Diaphragm and the lesser curvature is not continued upon it. The body and fundus (constituting about 5/6 of the entire organ) are on the left side of the body. The pyloric portion is notably less in caliber than the rest of the stomach; in the living it is separated from the body of the stomach by a sharp angle (angulus ventriculi) and is the only portion of the organ that lies to the right of the median line. In this region the musculature of the stomach wall is especially strong. Usually the pyloric portion is directed distinctly upwards and so approximates the cardia.
The musculature of the stomach consists exclusively of non-striated fibres and is arranged in general in three layers, which, however, are not all present in all parts of the stomach. The middle circular layer, which is also the strongest, extends over the entire stomach; at the pylorus it forms the pyloric sphincter. The outer longitudinal layer is developed chiefly along the curvatures and especially on the lesser curvature, but bundles spread out obliquely over the body and fundus, where they are gradually lost. It is directly continuous with the longitudinal musculature of the oesophagus. Only in the pyloric portion does it form an almost continuous layer, especially thick on the anterior and posterior surface, forming there the so-called pyloric ligaments. The innermost layer is termed the oblique layer. It is well developed only over the fundus and body and its fibres run obliquely from the left side of the cardia, at first almost parallel with the lesser curvature and then in an oblique direction, partly crossing with the fibres of the circular layer (see Fig. B57, B58).
The mucous membrane of the stomach, when that organ is contracted or partly so, presents folds, which bound small areas of the mucous membrane, the gastric areas, measuring 2-3 mm in diameter. At the pylorus the mucous membrane forms a circular fold, the pyloric valve and the so-called gastric canal in the region of the lesser curvature is bounded by longitudinal folds. At the cardia a zigzag line indicates the boundary between the epithelium of the oesophagus and that of the stomach. With a lens one can distinguish in the gastric areas the openings of the gastric crypts (foveolae).
(= Small Intestine 1, see here).
The duodenum is an almost horseshoe-shaped portion of the intestine, so placed that its convexity looks to the right and its concavity to the left. The head of the pancreas lies in the concavity. The duodenum begins at the pylorus of the stomach and extends to the duodenojejunal flexure; it has three portions, a superior, descending and inferior. It begins with the short, superior portion, which runs approximately from before backwards and at the same time horizontally and laterally, and passes into the almost vertical descending portion by the superior duodenal flexure. The descending portion is separated from the almost horizontal inferior portion by the inferior duodenal flexure, while the terminal part of the inferior portion, sometimes termed the ascending portion, bends upwards and to the left, passing across the median line.
In its structure the duodenum shows in general the typical characteristics of the small intestine, especially of the jejunum, yet the beginning of the superior part does not possess any circular valves (valvulae conniventes), these beginning shortly above the superior flexure. On the other hand, in this part which lacks the valvulae there are the duodenal (Brunner's) glands, most abundant towards the pylorus and usually disappearing shortly below the superior flexure. They are situated in the submucosa and are individually about the size of grains of millet.
In the descending portion are the orifices of the pancreatic ducts and the bile duct. The latter, the ductus choledochus, traverses the wall of the duodenum obliquely and forms a vertical fold of the mucous membrane, the longitudinal fold. At the lower end of this is the common opening of the bile duct and the greater pancreatic duct, which usually before reaching the opening forms a small enlargement of the fold, the duodenal diverticulum (greater duodenal papilla). The longitudinal fold crosses the circular valves at right angles; it is very low, but is the only longitudinal fold of the entire duodenum. It lies on the posterior medial wall of the duodenum. Somewhat higher, i.e. nearer the pylorus, on a small, wart-like elevation, the (lesser) papilla, is the opening of the lesser or accessory pancreatic duct; this and the papilla may be quite small or even occasionally wanting. The inferior portion of the duodenum differs only in its position from the jejunum, into the upper part of which its ascending portion passes over, without any demarcation, by the duodeno-jejunal flexure. At this flexure the duodenum is attached to the posterior body wall by a muscle bundle (the suspensory muscle of the duodenum, muscle of Treitz).
The small intestine, intestinum tenue, is a cylindrical tube about 6½ m in length, beginning at the pylorus of the stomach and ending by opening into the large intestine, gradually but markedly diminishing in diameter (from almost 4.5 to 2.5 cm) from above downwards. It consists of two principal portions: the duodenum (see here) and a freely moveable portion, the mesenterial intestine, so-called because it possesses a freely moveable mesentery, in contrast to the duodenum which is firmly fastened to the posterior body wall. In the mesenterial intestine two parts are recognized, the jejunum and ileum, which, however, pass into one another without demarcation. The wall of the intestine is quite thin. With the exception of the greater part of the duodenum it is surrounded by peritoneum, which forms the serous coat and is separated from the muscular coat by a thin subserous coat, which is free from fat except along the line of attachment of the mesentery. In addition there is a muscular coat, consisting of a continuous outer longitudinal layer and an inner circular one, a submucous and a mucous coat, the latter, like that of the entire digestive tract, possessing a lamina muscularis mucosae.
The mucous membrane of the small intestine, in addition to the tubular glands or crypts of Lieberkühn (intestinal glands), possesses villi throughout its entire extent, these giving to its interior a characteristic satiny appearance. Further the mucosa forms transverse folds, the circular folds (valvulae conniventes). These begin at about the superior duodenal flexure and extend to the lower end of the small intestine, becoming, however, gradually fewer and lower in the ileum, until they are either absent or merely scattered in its lower portion. The folds are to be seen only on the inner surface of the intestine and are for the most part, especially in the ileum, crescentic; only rarely do they completely surround the intestine. The mucous membrane of the small intestine is very rich in lymphatic tissue, especially in the ileum, and not only do individual lymph follicles (solitary nodules) occur, but also more or less extensive aggregations of these (aggregated nodules or Peyer's patches), these latter being found only in the ileum and only on the surface of this opposite the attachment of the mesentery. Frequently they are of considerable size, 10 cm or more in length, and their long axis coincides with that of the intestine.
The large intestine (intestinum crassum) is an almost cylindrical tube, of very variable width and 120-150 cm in length. It is divisible into two portions, the caecum with the appendix vermiformis and the colon, and forms a large horse-shoe-shaped loop, open below, surrounding the small intestine. Its general characters are as follows: it is the widest portion of the intestine; its caliber being greatest at the caecum and diminishing toward the rectum from 6-8 to 4-5 cm. Its wall, seen from without, in contrast with that of the small intestine, is not smooth, but presents outpouchings (haustra) produced by constrictions. These are due to the arrangement of three bands of longitudinal muscle fibres, the taeniae, which extend throughout the entire length of the large intestine. They begin on the caecum from a common area at the root of the vermiform appendix and extend over the wall of the intestine as smooth, shining bands, equally spaced and about 8 mm in breadth. One corresponds in position to the attachment of the mesentery and is termed the mesocolic taenia; that opposite is the free taenia and between these two is the omental taenia, so-called because it corresponds to the line of attachment of the great omentum to the transverse colon. The free taenia in the transverse colon is rather below than in front, as it is in the rest of the large intestine, and the omental taenia in the ascending and descending colons is on the lateral surface. If the taeniae are cut away or completely relaxed the haustra disappear. The outer surface of the large intestine is also characterized by the presence of subserous accumulations of fat, which form stalked, irregular, lobe-like appendages, the epiploic appendages. They are most abundant on the sigmoid colon and often are arranged in two rows, especially on the descending colon.
In the interior of the large intestine semilunar or sigmoid folds correspond to the constrictions between the haustra; as a rule each is as long as the interval between two taeniae, but they may be longer. In general the mucous membrane of the large intestine is smooth and not satiny, since it possesses no villi such as occur in the small intestine.
The caecum is that portion of the large intestine that is below the opening of the ileum. It is about 7 cm in length, is somewhat spherical and is the widest portion of the intestine. On its medial wall there is a valve at the entrance of the ileum, the valve of the colon (ileocaecal valve), formed by two folds of mucous membrane, the upper and lower lip (actually the entire wall is folded). These lips project into the caecum. From the lips semilunar folds pass to the anterior as well as the posterior wall; they run transversely like the semilunar folds, which they resemble except that they are longer. They are termed the anterior and posterior frenula.
The vermiform appendix (processus vermiformis) is a rudimentary, slender thin, blind appendage of the caecum, very variable in its development. It averages 7-9 cm in length, but may frequently be shorter or longer. It has neither haustra nor taeniae and in the child is merely the terminal portion of the conical caecum. In the adult it arises from the medial and posterior wall of the caecum and it is usually curved or slightly coiled. At its opening into the caecum there is a variable, valve-like crescentic fold of the mucous membrane, directed downwards and to the right, the valvule of the vermiform process.
The colon, the longest portion of the large intestine may be divided into four portions; a short, ascending colon, on the right side, arising directly from the caecum; a transverse colon running transversely or slightly upwards from right to left; a descending colon on the left side and a sigmoid colon connecting with the rectum. The last part, which is also on the left side, is, like the small intestine, arranged in several, usually two, loops, being moveable on account of possessing a mesentery. It lies, consequently, often in the neighbourhood of the caecum and very often in the true pelvis. Its length varies greatly (20-45 cm). At the junction of the ascending and transverse colons there is a bending of the intestine almost at right angles, the right or hepatic flexure, and at that of the transverse and descending colons there is a more acute left or splenic flexure. The descending colon is distinctly longer than the ascending.
The rectum extends from the sigmoid colon to the anus, arising from the sigmoid just below the promontory. Its length is about 15-16 cm. It is in general a cylindrical canal whose outer surface, in contrast to that of the colon, is smooth, so that it resembles the small intestine rather than the large. This is due to the fact that the taeniae of the colon spread out on the rectum, so that there is again a continuous and rather strong layer of longitudinal muscle fibres. The upper, greater portion of the rectum, situated in the true pelvis, the pelvic portion, is concave forwards, resting on the anterior surface of the sacrum; the lower, shorter perineal portion is convex anteriorly, bending around the tip of the coccyx, and passes through the musculature of the pelvic floor.
The inner surface of the rectum lacks the folds that characterize the colon, yet it does possess a variable number of transverse folds. One, rather constant and relatively high, is situated 8-10 cm above the anus, and in its region the circular musculature of the rectum thickens to form the so-called Sphincter ani tertius. Below this fold is a usually broader portion of the rectum, the rectal ampulla. In the lowest part of the rectum, the anal part, there are 6-8 longitudinal folds termed the rectal columns. They begin about 2-3 cm above the anus and end rather suddenly in the anulus haemorrhoidalis, a ridge immediately above the anal opening. Between adjacent columns there are corresponding depressions, the rectal sinuses. Both columns and sinuses gradually fade out above. The openings of the intestinal glands of the rectum are readily seen as fine points with a lens.
The actual (smooth) musculature of the rectum is very strong and in addition striated muscles are associated with the anal opening (see here). The longitudinal musculature ends at the upper border of the internal sphincter. The circular musculature at the lower end of the rectum close above the anus thickens over an extent of about 3 cm to form the Internal sphincter ani, composed of smooth fibres, in contrast to the transversely striated External sphincter ani. The wall of the rectum has a peritoneal covering only in its uppermost part and even there only on its anterior and part of its lateral surfaces.
The liver (hepar) is a brown-red organ, of friable consistence and of the form of a halved segment of a sphere; it weighs about 3 pounds. It has two principal lobes, a much larger right lobe and a smaller left lobe. There is a strongly convex superior surface, a posterior surface, also convex, and an inferior surface, for the most part concave. The superior and inferior surfaces meet in a sharp anterior border, while the small posterior surfaces passes over into both the large superior and the inferior surface without any definite boundary (see also here). On the under surface is the porta (portal fissure) which gives entry to the vessels and exit to the bile ducts. It lies almost at the middle of the inferior surface and is a transverse, deep and broad fissure. Into it pass the hepatic artery and the much larger vena portae, each as a rule already divided into its two principal branches, the right and left; further the nerves of the liver accompany the artery. From it emerges, usually by two main branches, the hepatic duct, which unites with the cystic duct to form the ductus choledochus (common bile duct) immediately before (below) the porta, and also a number of lymphatic vessels which pass to the (5-6) hepatic nodes (lymphoglandulae) situated in the porta. In addition to the transverse porta the inferior surface has two parallel sagittal fissures, which unite with the porta to form an H-shaped figure; these are the right and left sagittal fossae. The right one is broad and shallow and is divided at about its middle by the caudate process of the caudate lobe (see below) into an anterior fossa for the gall bladder and a posterior fossa for the vena cava. Also in the small left sagittal fossa two parts, which pass into one another at the left end of the porta, may be distinguished, an anterior fossa for the umbilical vein and a posterior fossa for the ductus venosus.
The left lobe of the liver, situated to the left of the left sagittal fossa, makes up only about one-quarter of the entire mass of the organ, but varies greatly in size and shows on its inferior surface a concavity produced by the stomach, the gastric impression, and a notch produced by the oesophagus, the oesophageal incisure. Only anteriorly and below does the surface show a convexity, the tuber omentale, which corresponds to the lesser curvature of the stomach. Its apex ends in the so-called appendix fibrosa.
The sagittal fossae with the porta bound the areas termed the quadrate lobe and the caudate (Spigelian) lobe, the former lying in front of the porta and the latter behind it. The caudate lobe is well defined by deep grooves on all sides, but it passes over into the right lobe by a small caudate process, which separates the two parts of the right sagittal fossa. Opposite this to the left is a rounded papillary process, which is covered by the peritoneum of the bursa omentalis and lies in the vestibule of that cavity.
The under surface of the right lobe shows a series of impressions of neighbouring organs. The largest of these is the renal impression for the right kidney; this is connected by the caudate process with the caudate lobe. Anterior to this is a duodenal impression and to the right of it and separated from it by a low ridge is the colic impression for the right colic flexure. The suprarenal impression is close beside the fossa for the vena cava. The quadrate lobe has a pyloric impression.
On the upper surface of the liver the falciform ligament, which encloses the ligamentum teres, indicates the boundary between the right and left lobes. At the anterior border there is an umbilical incisure, varying in depth. The posterior surface, in the region of the right lobe, has a rather broad area uncovered by peritoneum, which runs out into a small zone on the left lobe. The remaining parts of the liver, except the porta, are completely invested by peritoneum. The extensive, upper surface of the liver, which occupies the concavity of the diaphragm, is uniformly convex.
In sections of the liver, in addition to indications of the lobes, which are indistinct in the human liver owing to the absence of definite connective-tissue boundaries, one sees sections of its vessels. The branches of the hepatic veins lie isolated and are closely connected to the liver substance, so that they remain wide open and do not collapse, whereas the branches of the portal vein are surrounded by connective tissue, do collapse and are accompanied by branches of the bile ducts and hepatic arteries. Thus these vascular bundles are readily separable from the liver tissue on account of their connective tissue sheath (Glisson's capsule).
In the hepato-duodenal ligament the common bile duct lies most anteriorly and to the right, the hepatic artery with the nerves to the liver anteriorly and to the left, and behind these is the portal vein. In addition to some connective tissue, rich in fat, the two peritoneal layers of the lesser omentum also enclose in this region the hepatic lymph nodes (lymphoglandulae).
In the gall bladder (vesica fellea) one may distinguish the fundus from the more slender neck (collum), which passes gradually into the cystic duct. Between the two is the body (corpus).
The mucous membrane of the gall bladder even in the distended condition shows small folds, which unite to give a fine net-like appearance to the inner surface. The surface of the gall bladder which is not in contact with the liver is covered by peritoneum and the portion of the fundus that projects beyond the anterior border of the liver is completely enclosed by peritoneum.
The cystic duct is a short, irregular cylindrical canal which unites with the hepatic duct in the neighbourhood of the porta to form the common bile duct (ductus choledochus). Its mucosa is raised into peculiar folds, which have a somewhat spiral course and form a spiral valve (Heister's).
The spleen (lien) is a somewhat flattened organ with a large convex and a concave surface, the latter divided into subordinate areas. The convex diaphragmatic surface looks laterally, upwards and backwards and occupies the posterior, lower portion of the left cupola of the diaphragm. The other surface looks medially and is concave except for a slightly raised ridge in the long axis of the organ, on which is the hilus i.e. the pits for the entering vessels.
This ridge separates the medial surface into an anterior superior and a posterior inferior portion. The former is the gastric surface and the latter the renal surface. This has two not very distinctly separated areas, an upper, more strongly concave, for the upper end of the left kidney and a smaller lower, flatter one for the left flexure of the colon. The pits of the hilus are on the gastric surface, more or less close to the ridge, and in this region are also attached the peritoneal ligaments, the gastro-splenic (gastro-lienal) and the pancreatico-splenic (pancreatico-lienal). The superior extremity of the spleen is curved medianwards; the inferior extremity is directed downwards and to the left. The axis joining these two extremities is directed obliquely from above and behind, downwards and forwards. The posterior border of the spleen is usually smooth and rounded; the anterior border is sharper and has a number of indentations.
The spleen is not a gland (not even endocrine), but is a lymphadenoid organ interposed in the blood path and not in the lymph stream, as are the lymph nodes. It has, accordingly, no direct connection with the organs of digestion, but stands in relation to them in that its venous blood passes to the portal vein, of which the splenic (lienal) vein is a main tributary.
The spleen is enclosed in a rather strong, elastic capsule the tunica fibrosa, which sends into the interior of the organ strong trabeculae, which are plainly visible to the naked eye in sections (Fig. B84). They are distinctly thicker than the capsule and branch to form a fine network in the meshes of which is the soft substance, pulpa, of the spleen. This is of a dark red color, due to its blood content, since, in addition to large blood vessels which traverse it, it contains free red blood corpuscles, which undergo destruction in the spleen.
Scattered at rather regular intervals throughout the entire substance of the spleen are rounded bodies, the splenic (Malpighian) corpuscles (noduli lymphatici), which may be seen in sections by the naked eye (Fig. B84); they correspond to the secondary nodes of the tonsillar structures and the cortical portions of the lymph nodes. On account of their lighter, reddish-grey color they are readily distinguishable from the pulp tissue and have been termed the white or gray pulp.
The pancreas is a flat, elongated, lobed gland, situated transversely on the posterior body wall in front of the upper lumbar vertebrae. It presents three not clearly defined parts; the head (caput), the body (corpus) and the tail (cauda). The head lies in the horse-shoe shaped loop of the duodenum and is the broadest part of the gland. It almost completely fills the space enclosed by the duodenal loop and sends backwards and to the left a special curved process, the uncinate process (Fig. B87), which hooks around the superior mesenteric vein as this lies behind the pancreas in a groove, the pancreatic incisure. This groove separates the head of the gland from the body, forming a neck or isthmus.
The body (corpus) is the narrower, principal part of the gland and the tail (cauda) is its left end, usually extending to the spleen and being somewhat pointed. Three surfaces may be recognized in the pancreas, of which the inferior is small and is to be seen only on the body and even there is not clearly defined. The two principal surfaces, the anterior and posterior, are broad; the strongly rounded borders are superior, anterior and posterior. The anterior surface is covered by the peritoneum of the bursa omentalis, but the posterior surface is without a peritoneal investment and a part of the anterior surface of the head and the uncinate process also have no peritoneal covering. The anterior surface of the pancreas is not flat, but towards the right is distinctly convex, where it rests upon the bodies of the vertebrae and on the descending aorta in front of these; towards the left, on the other hand, it is distinctly concave as the result of its relations to the concave posterior surface of the stomach, this relation rendering it concave in the sagittal direction also. The anterior surface of the pancreas has therefore a saddle-like, if not an exactly saddle-shaped, form. The strongest projection of the upper border at the left edge of the convex portion is termed the tuber omentale and corresponds essentially to the lesser curvature of the stomach; it lies behind the bursa omentalis.
The pancreatic duct (Wirsung's) traverses the whole length of the gland, becoming larger from the tail to the head by receiving branches that enter it almost at right angles. It lies almost in the axis of the gland. In the upper part of the head of the gland there is an accessory pancreatic duct, whose relations are very variable. Usually it opens by a special orifice into the descending portion of duodenum, but it is always united by a transverse branch to the main duct and may open into this only.
The pancreas is not a purely exocrine gland, but also contains endocrine bodies, scattered like islands through the exocrine parenchyma and usually microscopic in size; they cannot, therefore, be seen by the unaided eye.
The peritoneum is a closed sac in which a parietal and a visceral layer may be distinguished, the latter covering the abdominal viscera that are invaginated into the sac. Between the two layers there is a cleft-like, complicated cavity, of extraordinarily small capacity and filled with a minimal amount of serous fluid. Where viscera are deeply invaginated into the peritoneal cavity the visceral layer passes to them as a double-layered mesentery, the nutrient vessels and the nerves being contained between the two layers of this.
The surface of the peritoneum is smooth and shining and confers these qualities on all the viscera it encloses, as well as on the abdominal walls, which are lined by the parietal layer.
If one studies the arrangement of the peritoneum in a median section (Fig. B105) one can trace the parietal peritoneum upwards upon the inner surface of the anterior abdominal wall until it passes without interruption upon the under surface of the diaphragm. From this it passes to the upper border of the posterior surface of the liver, (coronary ligament of the liver), and is continued over this as the visceral layer. To the right of the median plane and forming an acute angle with it a sickle-shaped duplicature, the falciform ligament, passes from the anterior abdominal wall (as far down as the umbilicus) and from the under surface of the diaphragm to the superior surface of the liver; in the lower free border of this duplicature the ligamentum teres, the obliterated umbilical vein, runs from the umbilicus to the under surface of the liver. Both layers of the falciform ligament pass over into the coronary ligament.
The liver is thus covered by peritoneum as far as the caudate lobe and on the under surface as far as the region of the porta; from there the peritoneum passes as the two layers of the lesser omentum to the lesser curvature of the stomach and to the upper surface of the superior portion of the duodenum (the hepato-gastric and the hepato-duodenal ligaments). In this manner the peritoneum reaches the stomach and the anterior layer of the lesser omentum is continued downwards over its anterior surface. From the greater curvature arise the anterior layers of the great omentum, an apron-like (quadruple) fold of peritoneum that hangs down over all the viscera of the lower part of the abdominal cavity (below the transverse colon and mesocolon). At the free, often lobed border of the great omentum its anterior layer coming from the greater curvature of the stomach passes over into the posterior layer and this attaches above to the transverse colon. It is then continued as the lower layer of the transverse mesocolon to be attached to the posterior abdominal wall in an almost transverse line.
Immediately below this line begins the root of the mesentery, which runs obliquely (from the left and above, downwards and to the right) across the lumbar portion of the vertebral column, supplying the peritoneal covering for all the mesenterial portion of the small intestine. Its line of origin passes at an acute angle into that of the transverse mesocolon; it begins opposite the left upper border of the second lumbar vertebra and extends to opposite the right sacroiliac articulation. After forming the usually very broad sigmoid mesocolon the peritoneum descends into the true pelvis, where it covers the upper part of the anterior wall of the rectum. Thence it is reflected in the male upon the bladder, in the female upon the fornix of the vagina and the uterus (see Fig. B108). From the bladder it then passes with the umbilical ligaments (Fig. B111) back to the anterior abdominal wall to become parietal peritoneum. There is a median umbilical ligament (= obliterated urachus) and two lateral umbilical ligaments (= obliterated hypogastric arteries).
The peritoneal pouch which is thus formed in the male between the rectum and the bladder is the recto-vesical pouch, while in the female, owing to the interposition of the uterus between the bladder and rectum, there are two pouches, the recto-uterine pouch between the rectum and the uterus or posterior fornix of the vagina and the vesico-uterine pouch between the uterus and the bladder. The widths of the rectovesical and recto-uterine pouches vary according to the extent to which the bladder and rectum are filled and they may be occupied by moveable portions of the intestine (loops of the small intestine or sigmoid colon); the vesico-uterine pouch in the normal anteflexed position of the uterus is always merely a capillary cleft.
By the umbilical ligaments and by the epigastric folds formed by the blood vessels of the same name, five shallow depressions are formed upon the anterior abdominal wall, the supravesical fovea, between the ligaments, and the paired medial and lateral inguinal foveae, separated by the epigastric folds.
The lateral inguinal fovea flattens out above and laterally, but its deepest point, where the epigastric fold crosses the inguinal (Poupart's ligament), marks the site of the abdominal inguinal ring. In the adult it is scarcely more than a slight depression.
The bursa omentalis is a deep pouch of peritoneum, which communicates with the general peritoneal cavity only by a relatively narrow opening, the epiploic foramen (foramen of Winslow). It lies chiefly on the left side of the body in the upper part of the peritoneal cavity.
The epiploic foramen (foramen of Winslow) lies, however, to the right of the median line, on the right edge of the hepato-duodenal ligament and, consequently, at the right edge of the lesser omentum; it is in the right wall of the bursa omentalis, more precisely, in the right wall of its less voluminous vestibule. It is an almost circular opening, lying almost in the sagittal plane. It leads into the vestibule of the bursa, whose anterior wall is principally formed by the lesser omentum; in this region the peritoneum of the bursa covers the caudate lobe of the liver, whose papillary process shows through the flaccid portion of the lesser omentum (the principal part of the hepato-gastric ligament). This part of the bursa is of slight depth and practically corresponds in width to the caudate lobe. In addition to the papillary process of the caudate lobe of the liver the tuber omentale of the pancreas usually shows through the lesser omentum.
In contrast to the small vestibule the principal portion of the bursa extends to the left between the posterior surface of the stomach and the anterior surfaces of the body and tail of the pancreas, as far as the spleen, and, furthermore, it dips down into the great omentum, forming its inner pouch. There is a constriction (isthmus) between the vestibule and the principal portion of the bursa, due to a fold of peritoneum, the gastro-pancreatic fold, caused by the left gastric artery and the coronary vein and extending from the upper border of the pancreas to the upper (left) end of the lesser curvature of the stomach.
That portion of the bursa omentalis which extends furthest to the left and reaches the spleen and its pedicles (the gastro-lienal and pancreatico-lienal ligaments) is termed the lienal (splenic) recess. The portion that descends into the great omentum is termed the inferior recess; it shows great individual variation and tends to become obliterated in its lower portion with advancing age. The process of the vestibule that extends upwards behind the posterior (upper) border of the caudate lobe of the liver to below the coronary ligament is termed the superior recess. The body and tail of the pancreas lie in the posterior wall of the main portion of the bursa, and above the pancreas this wall rests on the uppermost part of the anterior surface of the left kidney and on the left suprarenal gland (see Fig. B110).
The floor of the bursa is formed by the upper layer of the transverse mesocolon.
In addition to the bursa omentalis other pockets of the peritoneum, peritoneal recesses, occur, which are very variable both in number and in extent. These that occur most frequently are
In addition there are the pouches in the pelvis (see here).
The more important peritoneal folds and duplicatures (usually termed ligaments), most of which have already been described, are
The skeleton of the nose is formed only partly of bone, the rest is formed by the nasal cartilages. These consist of an unpaired cartilage, which forms the anterior prolongation of the osseous nasal septum, and a number of paired cartilages.
The cartilage of the septum; is a rather thin, irregularly quadrangular plate of cartilage, which is attached to the anterior edge of the vomer, the lower edge of the lamina perpendicularis of the ethmoid and the anterior part of the upper edge of the nasal crest. It ends in a free border a little above the nostrils, so that there is for a short distance a membranous nasal septum. The cartilaginous septum is usually bent either to one side or the other.
The lateral nasal cartilages appear to be direct prolongations of the septal cartilage, in that on the dorsum of the nose they fuse not only with one another but also with the upper part of the anterior edge of the septal cartilage. They are somewhat triangular and form the anterior lower part of the lateral wall of the nose. They are attached to the anterior borders of the nasal bones and to the frontal process of the maxillae by connective tissue. Below they do not reach the nostrils but unite with the alar cartilages.
The greater alar cartilages are two strongly curved strips of cartilage which surround the anterior part of the nostrils; each consists of a medial and lateral crus. The former is the smaller and is applied to the lower edge of the cartilage of the septum, lying in the membranous septum. The much stronger lateral crus forms the anterior part of the ala of the nose. The two crura are continuous at the tip of the nose.
The lesser alar cartilages are rather constant, small pieces of cartilage, frequently several in number, that lie above and behind the lateral crura of the two greater alar cartilages.
The nasal sesamoid cartilages are of frequent, but not constant, occurrence and are situated between the two greater alar cartilages and the lower borders of the lateral cartilages.
The cavity of the nose repeats, with but slight differences, the arrangement of the osseous nasal cavity. Only the anterior, lower portion has cartilaginous or membranous walls. It is divided by the septum into two symmetrical halves, each of which has an anterior opening at the nostrils (nares) and a posterior one, the choana, which leads into the pharynx.
In each cavity there are recognized a vestibule and the cavity proper, the respiratory region. The vestibule forms the transition between the external skin and the mucous membrane of the nose, and is separated from the cavity proper by a ridge, the limen nasi. Near the nares there are strong hairs, vibrissae, in the skin of the vestibule, and in addition sebaceous glands.
The boundaries of the actual nasal cavities are essentially the same as those of the bony cavity. Thus there are three conchae, superior, middle and inferior, covered with mucous membrane and containing the bony structures of the same names, but appearing more rounded than the bony ones on account of the mucous covering. Springing from the lateral wall of the cavity they divide the lateral part of the cavity into the three meatus, superior, middle and inferior, the remaining part of the cavity, between the free borders of the conchae and the septum, being termed the common meatus. The inferior meatus is between the inferior concha and the nasal surface of the hard palate, the superior between the middle and superior conchae.
The agger nasi, a slight elevation extending from the anterior end of the middle concha towards the tip of the nose, separates off, with the help of the anterior end of the inferior concha a flat area, the antrum of the middle meatus; this lies anterior to the middle meatus.
Above the superior concha, between it and the roof of the nasal cavity, there is a blindly ending recess, the spheno-ethmoidal recess, which does not extend back to the choanae but ends on the anterior surface of the body of the sphenoid bone. Sometimes a short uppermost concha occurs here, the concha suprema.
Since the two upper conchae are by no means as long as the nasal cavity, there is a common space in front of their front ends and behind their hinder ends; the anterior space has already been considered (see here); the posterior is the naso-pharyngeal meatus.
It lies immediately in front of the lateral border of the choana and is a shallow groove. Of the openings of the osseous nasal cavity there is a number that serve the passage of nerves and vessels and are closed by the mucous membrane of the nasal cavity, the spheno-palatine foramen for example. On the other hand there are others, such as the openings of the accessory cavities of the nose, that are evident in the cavity covered with mucous membrane. (Concerning these and the accessory cavities themselves see here). In addition, however, the following openings into the nasal cavity may be seen: In the inferior meatus, 2-3 cm from the nares and about 1 cm above the floor of the cavity, there is the inferior opening of the naso-lacrimal duct, which appears as a small slit partly covered by a small fold, the plica lacrimalis. Also in the floor of the cavity, beside the anterior end of the nasal crest, there is on either side an evagination of the mucous membrane into the incisive canal, the remains of an usually largely obliterated incisive duct.
Behind the opening of the incisive duct and above it there is usually in the mucous membrane of the septum of young individuals a slender, horizontal mucous canal, the rudiment of Jacobson's organ (vomero-nasal organ). It is usually well developed in the new-born child and is supplied by the olfactory nerve; in embryonic life it is fully established, although it later becomes quite rudimentary.
The uppermost portion of the nasal cavity, usually distinguishable by the darker color of its mucous membrane, is the olfactory region; it lies in the region of the superior concha and the uppermost part of the nasal septum, but is not sharply delimited from the respiratory region.
These have in general the same relations as the corresponding bony cavities. They are lined by a thin mucous membrane, poor in glands and united to the periosteum of the cavities, together with which it may be readily removed from the bone. They may be divided into the smaller and multiple ethmoidal cells and the larger single cavities, such as the frontal sinus, the sphenoidal sinus and the maxillary sinus. Like the principal cavity, these accessory cavities are paired.
The ethmoidal cells are divided by a frontal partition into an anterior and a posterior group. The larger and less numerous (2-3) anterior cells open into the middle meatus, being separated from the infundibulum (see below) by the ethmoidal bulla, a convex prominence of the lateral nasal wall. The cells of the posterior group, smaller and more numerous (3-4) than those of the anterior group, open into the superior meatus usually by several separate openings. The various anterior and posterior cells communicate with one another, but there is no communication between the two groups a thin, bony partition in the frontal plane separating them. They are interposed between the orbital and nasal cavities, forming what is termed the ethmoidal labyrinth. The most anterior of the large anterior cells often comes into close relationship with the frontal sinus, being separated from it only by a thin plate of bone.
The frontal sinuses lie in the nasal portion of the frontal bone, but when they become enlarged they extend into the frontal plate and even into the orbital portion. Towards the nasal cavity each sinus narrows so as to become duct-like (the infundibulum) and opens into the middle meatus, in reality into the upper anterior portion of the hiatus semilunaris, a groove-like depression of the lateral nasal wall below the ethmoidal bulla (see here).
The sphenoidal sinuses lie in the anterior portion of the body of the sphenoid bone; the two cavities are separated only by a very thin partition, usually not quite in the median line. The cavities of the two sides open anteriorly, close together, in the spheno-ethmoidal recess, by rather wide openings; the adjacent optic nerve and internal carotid artery cause elevations in the walls of the cavities.
The maxillary sinuses (antra of Highmore) are the largest of the nasal accessory sinuses. They lie on each side of the lower (and middle) portion of the nasal cavity, beneath the orbits and immediately above the mouth cavity; they are bounded on almost all sides by only very thin bony walls. In each sinus the neighbouring nasolacrimal canal produces an elongated elevation of the medial wall and in the floor the roots of the molar teeth form the so-called alveolar tubercles. The opening of the sinus into the nasal cavity is in the middle meatus; it is a slit-like opening, behind the opening of the frontal sinus in the posterior part of the hiatus semilunaris; in addition a roundish accessory opening, also into the middle meatus below the hiatus, may occur, but it is not constant.
The thyreoid cartilage, much the largest of the laryngeal cartilages, consists of two symmetrical, almost quadrangular plates, which are fused together at a right angle (obtuse in the female) in the median line by their anterior edges, forming the laryngeal protuberance. Above the line of fusion there is a deep superior notch (incisura) and below it a very slight inferior notch (incisura). The posterior edges of the two plates are widely separated and the almost straight posterior border of each is prolonged above and below into a process. The superior cornu is the longer and is curved somewhat inwards and backwards; the inferior cornu is shorter and curved forwards and inwards; it bears an articular surface for the cricoid cartilage.
The inner surface of the thyreoid cartilage is smooth, but the outer has an elevation, the superior tubercle, near the posterior part of its upper border. From this an oblique line runs downward and medially to an inferior tubercle on the lower border. The cricoid cartilage has the form of a seal ring, whose broader part, the lamina, is behind and the narrower part, the arch (arcus), in front. The lower borders of the lamina and arch are at about the same level so that the upper border of the arch slopes upward to the lamina. On the outer surface of the arch in the region of its passage into the lamina there is an articular facet for the inferior cornu of the thyreoid cartilage. The lamina is three times as high as it is thick and on its upper border it bears articular facets for the arytaenoid cartilages.
The cartilage of the epiglottis is a thin plate, convex above and in front, concave below and behind. It bears on its posterior surface a ridge (carina) and tapers off below into a narrow stalk (petiolus), which fastens into the superior incisure of the thyreoid cartilage. It shows numerous small depressions or even perforations.
The arytaenoid cartilages are two in number, each having the form of a triangular pyramid. The base has a concave articular facet for articulation with the upper border of the lamina of the cricoid and its anterior angle is prolonged into a pointed process, the vocal process, while the blunter lateral angle is the muscular process. The lateral surface has a curved ridge, the arcuate crest, which begins at the vocal process and passes at first backward and then upward; it separates an upper triangular fovea from a lower oblong fovea. Above the latter, near the anterior border is a rounded tubercle, the colliculus. The posterior surface is concave and the medial, almost flat, is situated in the median plane.
The corniculate cartilages (cartilages of Santorini) are small, pyramidal bodies, seated upon the apices of the arytaenoid cartilages. They are directed backward and medianward. The cuneiform cartilages (cartilages of Wrisberg) are rod-like cartilages situated in the ary-epiglottic folds near the anterior border of the arytaenoid cartilages; they are inconstant. The roundish cartilagines triticeae are also inconstant, but may occur in the lateral hyo-thyreoid ligament.
The paired crico-thyreoid articulation is between the inferior cornua of the thyreoid cartilage and the arch of the cricoid. Each is enclosed by an articular capsule and has as reinforcing bands the lateral, posterior and anterior cerato-cricoid ligaments.
The crico-arytaenoid articulation, also paired, is between the base of an arytaenoid cartilage and the upper border of the lamina of the cricoid. The thin articular capsule is reinforced posteriorly by the strong posterior crico-arytaenoid ligament.
The ary-corniculate synchondrosis is the articulation of the corniculate and arytaenoid cartilages. The lax elastic hyothyreoid membrane unites the upper border of the thyreoid cartilage to the lower border of the body of the hyoid bone and to its greater cornua. It is perforated laterally by an opening for the passage of the superior laryngeal nerve. Its middle, firmer portion is termed the middle hyo-thyreoid ligament, while the lateral portions, which unite the tip of the greater cornua of the hyoid bone to the superior cornua of the thyreoid cartilage, are known as the lateral hyo-thyreoid ligaments. These frequently contain the cartilagines triticeae. On the hyo-thyreoid membrane there is on either side, close to the middle hyo-thyreoid ligament, a constant, flat, lobed mass of fat. The cricoid cartilage is attached to the neighbouring trachea by the crico-tracheal ligament.
From the tips of the corniculate cartilages an elastic band of fibres extends downwards on either side and unites with that of the other side at the upper border of the lamina of the cricoid cartilage; it is in relation with the mucous membrane of the pharynx, which covers it, and is therefore termed the corniculo-pharyngeal ligament.
The Crico-thyreoideus arises from the outer surface of the arch of the cricoid cartilage and is inserted into the lower border and inferior cornu of the thyreoid cartilage. It has a superficial straight and a deep oblique portion.
The Crico-arytaenoideus posterior arises from the posterior surface of the lamina of the cricoid cartilage and inserts into the muscular process of the arytaenoid cartilage.
The Crico-arytaenoideus lateralis arises from the lateral part of the arch of the cricoid and is inserted into the muscular process of the arytaenoid.
The Arytaenoideus transversus arises from the lateral border and posterior surface of one arytaenoid cartilage and passes to the corresponding parts of the other.
The Arytaenoideus obliquus arises from the muscular process of one arytaenoid and passes to the apex of the other.
The Ary-epiglotticus, variably developed fibres in the ary-epiglottic fold.
The Thyreo-arytaenoideus arises from the inner surface of the thyreoid cartilage and inserts into the muscular process and lateral surface of the arytaenoid cartilage. Those fibres that are contained within the vocal fold are sometimes termed the m. vocalis. The Ventricularis consists of fibres lying in the false vocal fold (plica ventricularis).
The Thyreo-epiglotticus is formed by prolongations of the thyreo-arytaenoideus into the ary-epiglottic fold.
The Crico-thyreoideus is supplied by the superior laryngeal nerve, all the other muscles by the inferior laryngeal. The Crico-thyreoideus tenses the vocal cords and the Thyreo-arytaenoideus relaxes them; the Crico-arytaenoideus posterior widens and the lateralis narrows the rima glottidis. The remaining muscles act as constrictors of the entrance to the larynx and of the rima glottidis, or, as in the case of the m. vocalis, regulate the tension of the vocal cords.
The epiglottis is fastened by its anterior surface to the upper border of the body of the hyoid bone by the broad hyoepiglottic ligament and the petiole is seated in the superior thyreoid notch by means of the thyreo-epiglottic ligament.
On the outer surface of the larynx there is a strong elastic band, the crico-thyreoid ligament, which connects the inferior thyreoid notch with the upper border of the arch of the cricoid cartilage; it forms the anterior end of the elastic cone.
This is an especially strong portion of the elastic lining of the larynx; it lies immediately beneath the mucous membrane and has the form of a short conical tube. It begins at the upper border of the cricoid cartilage and extends upwards, diminishing in size, to the arytaenoid cartilages and to the vocal cords (vocal ligaments), which are paired thickened strips of the elastic cone and arise close together from the inner surface of the angle of the thyreoid cartilage. They pass backwards, almost parallel with one another and close to the median line, to the vocal process of the arytaenoid cartilage. Above and parallel with them are the weaker, less elastic, but somewhat longer false vocal cords (ventricular ligaments).
The mucous membrane of the larynx follows as a whole, even as to individual folds, the relief of the skeleton of the larynx and of the elastic cone. The epiglottis is attached to the tongue by the median and lateral glosso-epiglottic folds, between which, on either side, there is a depression, the epiglottic vallecula. Furthermore, from the epiglottis two folds, the ary-epiglottic folds, pass backward to the tips of the arytaenoid and corniculate cartilages and form the lateral boundaries to the entrance (aditus) of the larynx; in addition to muscle fibres (ary-epiglottic) they usually contain the cuneiform cartilages. Upon each of them are to be seen two knob-like elevations of the mucous membrane, one, the corniculate tubercle, over the corniculate cartilage and the other, the cuneate tubercle, over the cuneiform cartilage.
From the entrance to the larynx the mucous membrane extends down into the actual cavity of the larynx, which it lines. The most important structure shown by the mucosa in this region is the vocal organ, the glottis. It lies at about half the height of the larynx and consists of the two vocal lips (labia vocalia) and the rima glottidis. The vocal lips are formed by the mucous membrane covering the vocal cords and the vocal muscles; their free borders are termed the plicae vocales. Posteriorly they contain the vocal processes of the arytaenoid cartilages. The glottis divides the cavity of the larynx into two portions, an upper vestibule and an inferior cavity of the larynx.
The rima glottidis is divided into a short posterior, but wider intercartilaginous part, bounded laterally by the vocal processes of the arytaenoid cartilages and the mucous membrane covering them, and a longer, anterior and narrower intermembranous part, bounded laterally by the vocal ligaments and the mucosa covering them. Both parts are quite distinct when in the relaxed condition (as in the cadaver), since the tips of the vocal processes show through as yellowish points. At the anterior part of the vocal lips, just before their attachments to the thyreoid cartilage, there is a constant yellow spot (macula flava).
The false vocal folds (plicae ventriculares) are folds of mucous membrane parallel to the vocal lips. They are formed by the mucous membrane covering the false vocal cords (ventricular ligaments and muscles). Between their free edges there is a relatively wide cleft, the rima vestibuli, whose width is not alterable. In the phonation position it is markedly wider than the rima glottidis, so that on looking into the entrance of the larynx one can see the vocal lips. Between the true and the false vocal folds there is a lateral evagination of the laryngeal cavity, the ventricle of the larynx (ventricle of Morgagni), from the upper wall of which a blind prolongation, the appendix of the ventricle, extends upwards behind the anterior end of the false vocal cord to the posterior surface of the thyreoid cartilage. The mucosa of the portion of the larynx below the glottis covers smoothly the elastic cone. The part of the cavity immediately below the glottis is termed the inferior entrance (aditus) of the glottis. In the vestibule on the anterior wall there is an epiglottic tubercle corresponding to the base of the petiole of the epiglottis.
The trachea is a rather firm tube, 10-20 cm long and 11-18 mm in diameter. It takes origin from the larynx opposite the fibrocartilage between the sixth and seventh cervical vertebrae and extends to the level of the fibrocartilage between the fourth and fifth thoracic vertebrae. At this level or that of the fifth thoracic vertebra, it divides almost at a right angle, into the two bronchi, of which the right bronchus is the wider but shorter and the left bronchus the narrower, longer and steeper. The left bronchus forms with the median line an angle of about 45° and the right an angle of 25°.
The skeleton of the trachea consists of 16-20 cartilaginous rings, the tracheal cartilages, which are open behind. They form the anterior and lateral walls of the trachea, while the posterior wall contains no cartilaginous skeleton but consists mainly of smooth muscle fibres which extend between the ends of the rings.
The thyreoid gland is one of the ductless glands. It lies in the neck in front of the upper part of the trachea and in front of the lateral parts of the lower portions of the larynx. In its middle portion it is covered by the superficial and deep layers of the cervical fascia, in its lateral portions by the two Sternothyreoid muscles, which lie directly on the gland, and by the other infrahyoid muscles.
It is unpaired, has a horseshoe shape and consists of a small median portion, the isthmus, and two lateral lobes.
The flattened isthmus lies in front of the upper three or four tracheal cartilages and, when well developed, also in front of the crico-tracheal ligament and the arch of the cricoid cartilage. In correspondence with the form of the trachea it is convex in front and concave behind. Not infrequently an unpaired, usually flat process, the pyramidal lobe, arises from it, extending upward to the body of the hyoid bone and tapering as it goes.
The much more voluminous and markedly thicker lobes lie to the sides of the lower portion of the larynx and the upper portion of the trachea. Below their ends are rounded and do not extend much below the level of the lower border of the isthmus, but above they end in strongly rounded tips considerably above the upper border of the isthmus. Behind they reach the lateral walls of the laryngeal portion of the pharynx and the upper portion of the oesophagus. Frequently the two lobes differ in size.
The surface of the gland usually appears distinctly lobed, its color is grayish red and in section it shows fine vesicles, filled with colloid, which appear as dots or of the size of millet seed.
Frequently there is a more or less distinct line of separation between the lobes and the isthmus and in other respects also the isthmus seems to possess a certain independence of the lobes, being occasionally quite rudimentary or even entirely absent.
In addition to the main gland there are occasionally accessory thyreoid glands, which are to be regarded as portions of the inconstant pyramidal lobe. They sometimes extend up to the hyoid bone. Not to be confused with these are the parathyreoid glands which are constant epithelial bodies, two or three in number, situated on the posterior surface of the lobes of the thyreoid gland, on branches of the inferior thyreoid artery. They are only topographically related to the thyreoid gland, and lie outside its connective tissue capsule.
The pyramidal lobe, which not infrequently occurs as a variation, is to be regarded as the remains of the original embryonic duct of the gland. Since the foramen caecum of the tongue and the thyreo-glossal duct that occasionally continues this deeply, mark the spot from which the embryonic gland arises, the pyramidal lobe also often extends upwards to the hyoid bone. As a result of the partial degeneration of the pyramidal lobe the frequently occurring accessory thyreoids (see here) are formed.
The thyreoid gland is enclosed within a connective tissue capsule, which takes origin from the cervical fascia; it sends septa into the substance of the gland, dividing it into various lobes. By means of this capsule and ligamentous prolongations from it the gland is attached to the cricoid cartilage and to the upper rings of the trachea; two lateral ligaments, which attach the medial surfaces of the lateral lobes to the trachea, are stronger than a middle one, passing to the posterior surface of the isthmus. The parathyreoid glands (see here) are altogether outside the capsule of the thyreoid.
In addition there may be suspensory muscles of the thyreoid gland; as a rule these are aberrant fibres of the Cricothyreoideus or Thyreo-hyoideus (more rarely of the Constrictor inferior of the pharynx).
There are two lungs, a right (pulmo dexter) and a left (pulmo sinister). They are quite similar, but the right is more voluminous than the left, although the latter is higher (longer).
The base of the lung is a strongly concave surface, the diaphragmatic surface, resting upon the cupola of the diaphragm. The rounded apex, directed upwards, has, in the case of the left lung, a shallow, broad groove for the subclavian artery on its medial surface.
The extensive, convex surface which is turned towards the ribs and is directed mainly laterally is termed the costal surface, while that opposite, the smaller medial and mostly concave surface facing the heart, is the mediastinal surface. The costal and diaphragmatic surfaces are separated by a very sharp inferior border; the mediastinal and lateral surfaces by the also thin but less smooth anterior border.
The mediastinal surface of the lung, which is practically in the sagittal plane, shows at about its middle and towards the anterior border a cardiac impression. Owing to the asymmetrical position of the heart this is necessarily greater on the left lung than on the right one. The portion of the surface behind the impression is in part convex, but shows a vertical furrow, which in the left lung is due to the aorta and in the right to the vena azygos.
In the posterior part of the cardiac impression there is a slightly depressed, pear-shaped area, with its small end directed upwards; it is the hilus and gives entrance to the vessels and bronchi. The surface of the lung up to the hilus is covered by peritoneum, the pleura, and is therefore smooth as glass. On the reddish-grey surface dark, blue-black to black lines (coal dust deposits), which mark out the individual pulmonary lobules, may be seen and, further, certain deep fissures, the interlobar incisures, which separate the various lobes and pass deeply into the substance of the lungs. The pleura extends into the depth of the interlobar fissures, even almost to the hilus, so that the individual lobes are continuous only to a small extent. The fissure between the middle and upper lobes of the right lung is not so deep as the others (see here).
The larger right lung is divided by two fissures into three lobes, upper, middle and lower; the smaller left lung on the other hand has only an upper and lower lobe, corresponding to the occurrence of only one interlobar fissure. This runs obliquely from behind and above, downwards and forwards, beginning above at the level of the third rib and ending at the lower border of the lung in such a manner that the most anterior portion of the border belongs to the upper lobe. The fissure is to be seen on the costal and mediastinal surfaces (except at the hilus) and for a slight extent also on the diaphragmatic surface. Of the interlobar fissures of the right lung that which separates the upper and middle lobes from the lower one corresponds in its position to the fissure of the left lung, except that above and behind it begins a little lower down and reaches the base and the lower border further lateral than in the left lung. This fissure is markedly deeper than the other one of the right lung and is to be seen on the costal, mediastinal and diaphragmatic surfaces. The second fissure of the right lung, separating the upper and middle lobes, is shorter than the other and at the same time shallower, and is almost at right angles to it. It is visible only on the costal and the anterior part of the mediastinal surface, and not at all on the diaphragmatic surface. The upper lobe on the right lung consequently does not reach the base of the lung as does that of the left lung. The anterior border of the right lung is almost straight, but that of the left lung has an incision, the cardiac incisure, which allows the pericardium to be seen. The lower, anterior end of the upper lobe of the left lung projects below this incisure into a small tongue-like lobe, the so-called lingula, which rests on the pericardium.
The hilus of each lung remains free from investment by the pleura; from its lower end the attachment of the ligamentum pulmonale extends downwards. In the hilus, in addition to the vessels, nerves and bronchi which form the root (radix) of the lung, there are also small pulmonary lymph nodes (lymphoglanduae). The vessels and the bronchi are so arranged at the hilus that the branches of the pulmonary artery are placed most anteriorly and the bronchi most posteriorly and below; only in the right lung is there an eparterial bronchus (see here). The nerves accompany the branches of the bronchi.
Even before the bronchi reach the hilus of the lung they begin to give off branches (rami), which are divisible, according to their relation to the pulmonary artery in the hilus, into eparterial and hyparterial branches. Only the branch to the upper lobe of the right lung is eparterial, i.e. it passes into the lung above the branch of the pulmonary artery, while the rest of the bronchial rami of the right lung and all those of the left lung are hyparterial, i.e. they lie at the hilus below the branches of the artery.
The further branching of the bronchial rami takes place within the lung. As the branches diminish in caliber longitudinal folds of the mucous membrane, quite lacking in the larger branches, become more and more evident and more numerous; in the smallest branches these folds are exceptionally distinct. The branching of the bronchi in the lungs is irregularly dichotomous; an actual so-called stem bronchus, which represents the continuation of the main bronchus, cannot be distinguished. In the branches of the bronchi the cartilaginous rings which characterize the trachea and bronchi give place to irregular cartilaginous plates and the finest branches, those with an average diameter of 0.5 mm or less, have no cartilage in their walls and are termed bronchioles.
Sections of the lung reveal, in the first place, the boundaries of the individual lobuli, formed by delicate strands of connective tissue and, secondly, sections of the bronchial rami and the larger vascular branches. It is a rule that the arterial and bronchial branches run together, while the stronger branches of the veins pursue a different course. The bronchial branches are distinguishable from those of the arteries by the occurrence in their walls of plates of cartilage. Very frequently there are deposits of black pigment (carbon particles) in the peribronchial connective tissue.
In the individual lobules sections of the alveoli as well as those of the bronchioles can be seen with the aid of a lens; they are not visible to the naked eye. A bronchiole of the first order passes to each of the lobuli.
The thymus gland is a peculiar glandular (perhaps only gland-like) organ, which is much more strongly developed in young individuals than in adults. It shows its relatively greatest size in the new-born child; then its growth becomes retarded, although until puberty it increases in absolute size. Thereafter a complete cessation of growth occurs to which succeeds a gradual process of degeneration, which does not, however, lead to a complete disappearance of the gland, even in the adult; as a rule it no longer appears as a compact organ but is extensively infiltrated with fat tissue (see here).
Actually it is a paired organ, but the two glands come to lie with their medial surfaces in close apposition, so as to give the impression of an unpaired organ consisting of two lobes. Technically a right and a left lobe, separated completely by connective tissue, by fat tissue in the adult, are recognized.
It is a flat organ of a clear grayish-red color and of rather soft consistency; its contours may be very irregular, since frequently more or less deep notches extend into the gland. The lobation of the gland is always well marked, the lobules being separated by strands of connective tissue. All the lobes, however, are originally connected by a fine central cord of gland tissue, the central tract; later, with the development of fat tissue and the consequent separation of the lobules, this connection disappears. The upper end of the organ is often drawn out into a slender prolongation and may then extend into the neck; below the gland becomes distinctly broader. Like the thyreoid gland it belongs to the category of ductless glands (glandulae clausae) and in its development it is closely related to the parathyreoid glands.
The thymus is about twice as long as it is broad and it is flat up to its middle broadest portion. On the posterior surface it appears to be distinctly concave, lying as it does on the convex pericardium. It is situated in the upper portion of the superior mediastinum, behind the manubrium and upper portion of the body of the sternum; in childhood, however, it rests broadly on the anterior surface of the pericardium and extends into the anterior mediastinum. It also lies in front of the left innominate vein, between the vein on the one side and the manubrium and upper part of the body of the sternum on the other; it lies, accordingly, in front of the arch of the aorta and its great branches and, in the child, also between the two anterior mediastinal laminae, which rest upon the lateral surfaces of the organ. The upper, elongated ends of the thymus lobes often extend into the neck, even to the thyreoid gland but, are, as a rule, only poorly developed.
The remains of the thymus in the adult, strongly infiltrated with fat, reaches neither by its upper nor its lower end the levels attained by the thymus of the child, which appears as a compact glandular mass often only to the twelfth year. That shown in Fig. B152 is an exception. At the most it reaches the apex of the pericardium, no longer, as in the child, extending upon its anterior surface, since in the adult the growth of the gland lags markedly behind that of the heart. It is consequently limited in the adult usually to the anterior portion of the superior mediastinum, where it lies imbedded in the so-called retrosternal fat body. Occasionally, however, even in the adult, the thymus forms a compact mass within the mediastinal fat tissue (Fig. B152). With advancing age the remains of the gland become more scattered and more and more atrophic, so that by the 60th year usually no thymic tissue persists.
The kidneys (renes) are two paired organs resting on the posterior abdominal wall. Each has a strongly convex anterior and posterior surface, separated by rounded medial and lateral borders, the latter being convex, while the former at its middle is concave to form the hilus. The rounded ends are superior and inferior. The surfaces of the kidneys show faint impressions of the neighbouring organs, a muscular impression on the posterior surface for the Quadratus lumborum and the hepatic impression on the anterior surface, the left kidney having also gastric, pancreatic, colic and splenic (lienal) impressions.
The hilus serves for the entrance of vessels and of the ureter, the latter being below and behind the vessels, and of these the artery is behind the vein. The hilus leads into a cavity, the renal sinus, surrounded by kidney substance. It has the form of the kidney and contains much fat tissue, the branches and the roots of the ureter, the calices and pelvis. The kidney is covered on its outer surface by a fibrous tunic or capsule and its substance consists of two portions, a cortical and a medullary substance. The former constitutes the whole of the surface of the kidney, while the medullary substance is formed by the renal pyramids, whose bases connect with the cortical substance, while their apices project as the renal papillae into the renal sinus. The papillae are 7-12 in number, the pyramids 15-20. At the apex of each papilla the straight urinary canals, the ductus papillares, open by minute foramina papillaria (area cribrosa). Between the bases of the renal papillae portions of the cortical substance, the renal columns (Bertini), descend to the sinus and between them and the pyramids the stronger branches of the blood vessels enter or leave the kidney substance. The kidneys of the fetus and of the new-born child are distinctly lobed.
The excretory duct system of the kidney begins at the renal sinus as the renal calices, which, on the one hand, are attached to the lateral borders of the papillae and at the other pass into the renal pelvis, an enlargement of the ureter (see below) in the sinus and usually also in the region of the hilus. Usually several calices unite to form a single stem before they reach the pelvis and accordingly greater and lesser calices are recognized. The number of the latter corresponds with that of the papillae; that of the greater calices varies greatly. The renal pelvis corresponds in shape to the renal sinus and is a short flattened, somewhat funnel-shaped tube, but shows, however, much individual variation.
The ureter is an almost cylindrical canal 30 cm in length. It begins at the apex of the renal pelvis and terminates by opening into the lower posterior part of the bladder. It has an abdominal and a Pelvic portion. In the empty state it is flattened; its musculature is weak, so that its walls are lax. In the distended condition it has the caliber of small pencil; it is somewhat narrowed in its pelvic portion and just above this narrowing there is a spindle-shaped enlargement.
The suprarenal glands are paired, ductless glands, seated on the upper ends of the kidneys. The left one has usually a somewhat crescentic form, while the right is more triangular, the apex being upwards. Each has an anterior and posterior surface and the concave surface in contact with the kidney is the base. Each has also a medial and a superior border and the right one has an apex. On the anterior surface there is a shallow groove, the hilus, where vessels and nerves enter or leave the gland.
Sections through the gland show that it is composed of a compact, yellow or brownish cortical substance, completely enclosing a soft, grayish-red medullary substance. The latter, in addition to numerous nerves, contains large blood vessels, their lumina being visible to the naked eye in sections.
The urinary bladder (vesica urinaria) is an unpaired bladder-like structure in which the upper part, which is conical in the new-born child, is termed the vertex, the middle part the body and the lower part, turned towards the perineum, the fundus. When full it is usually ellipsoidal, but when completely emptied it is almost spherical, or, in the female, bowl-shaped by being compressed by the uterus above. From the vertex the middle umbilical ligament arises, this being the remains of the embryonic urachus. In the new-born child it still shows remains of a lumen.
The bladder has three orifices, those of the two ureters and that of the urethra. They lie within 1-2 cm of one another at the fundus, the urethral orifice at the lowest portion of the bladder, those of the ureters in the lower part of the posterior wall. The ureters traverse the wall of the bladder obliquely and so produce two converging folds, the ureteric folds, which are continued beyond the orifices for some distance, gradually fading out. Further the two ureteric openings are connected by a low transverse elevation, so that there is formed a triangular area, the trigone, at each of whose angles one of the orifices is situated and whose surface is smooth even in contraction, whereas the surface of the rest of the organ is rugose. Usually a ridge, the uvula, extends from the apex of the trigone to the urethral orifice.
The wall of the bladder consists of the mucous membrane, a muscular coat and a serous coat, which, however, covers only the upper surface up to the apex and the upper parts of the lateral surfaces, being reflected posteriorly upon the rectum in the male and upon the uterus in the female. It does not extend over the posterior wall beyond the upper ends of the seminal vesicles in the male. The muscular coat consists of three layers. The outer one consists mainly of longitudinal fibres. The middle one is the strongest of the three and consists of an almost continuous sheet of circular fibres, which become more oblique in the upper part and have an almost transverse direction in the lower part. A thickening of the layer at the urethral orifice is the anulus urethralis and serves as a sphincter of the bladder. The inner muscular layer is a net-like, wide-meshed sheet, immediately beneath the mucosa; the fibres have a general longitudinal tendency.
The prostate is a glandulo-muscular structure, situated at the lower end of the bladder. It is of firm consistence and is a thickening of the upper part of the wall of the urethra, so arranged that it is thinner and lower anteriorly and thicker and higher posteriorly. The broad, upper surface united to the bladder is the base, and the strongly rounded apex is directed downwards and forwards. A slight furrow on the posterior surface divides the chief mass of the gland into two imperfectly separated portions, the right and left lobes. A transverse groove, due to the entrance of the ejaculatory ducts, separates an anterior lobe, termed the isthmus. The posterior surface is almost flat, the anterior surface is much shorter and almost vertical. The two surfaces pass into one another by rounded convex lateral surfaces. The prostate is distinctly flattened from before backwards. Half of its substance is smooth muscle tissue, the m. prostaticus, and the other half is gland substance. This is made up of a number (30-50) of individual glands, all imbedded in the muscle tissue and opening, by about 10-15 prostatic ducts, into the prostatic portion of the urethra. In correspondence with the stronger development of the glands in the posterior portion of the organ, the orifices of the ducts are mainly on the posterior wall of the urethra, especially on the lateral slopes of the colliculus seminalis and in the groove alongside it; the thin part of the organ situated in front of the urethra is destitute of glandular tissue.
The testis is a paired, ellipsoidal structure, enclosed in the scrotum in a special serous covering. It has a superior and an inferior extremity and lateral and medial surfaces, the latter being separated by well rounded anterior and posterior borders. The testis is covered by a firm, white capsule of connective tissue, the tunica albuginea, which is pierced towards the posterior border of the testis for the entrance and exit of vessels and nerves. The posterior border is consequently fixed, while the anterior one is free. In addition there is on the posterior border a keel-shaped mass of connective tissue, triangular in section, the mediastinum testis, whose sharp anterior border projects into the substance of the testis. It is decidedly shorter than the testis, gradually fading out both upwards and downwards, and from it horizontal and sagittal connective tissue partition walls, the septula testis, pass radially towards the tunica albuginea. The lobules of the testis between these contain the seminiferous tubules, slender, much curved and contorted, white tubules, large enough to be seen by the naked eye. In the mediastinum they pass into straighter, much narrower, anastomosing tubules, the tubuli recti, which form the rete testis. From the base of the mediastinum 10-15 efferent ducts emerge to pass into the head of the epididymis.
The epididymis is a long, club or retort-shaped body, which extends along the entire length of the posterior border of the testis. In its middle portion, the body (corpus), it is triangular-prismatic, but becomes enlarged and rounded at its upper end to form the head (caput), while its lower end is termed the tail (cauda). The head is directed medially and its under surface rests on the upper end of the testis. The body is distinctly prismatic and is the narrowest portion of the structure; its anterior border is firmly connected with the posterior border of the testis and the adjacent part of its lateral surface, but otherwise it is separated from the testis by the sinus epididymidis. The distinctly flattened, curved tail lies at the lower end of the testis and bends sharply into the more posterior ductus deferens, which runs upwards.
In the head of the epididymis the efferent ducts of the testis become much contorted, forming the conical lobuli epididymidis and these unite with an exceedingly long ductus epididymidis, which is very greatly contorted, its closely appressed coils forming the body and tail of the epididymis. At the end of the tail this duct, gradually ceasing to be coiled, becomes continuous with the ductus deferens. The testis and epididymis are contained within a serous membrane, the tunica vaginalis, whose visceral layer covers the testis completely, except over the area where the vessels enter, and the epididymis partly, being reflected from the head and tail of the latter to the posterior surface of the testis, forming the superior and inferior epididymal ligaments. Between these and between the body of the epididymis and the testis is a cleft-like pouch of the vaginal cavity, the sinus epididymidis. On the upper end of the testis, and like it covered by the tunica vaginalis, is an appendage, the appendix testis (sessile hydatid), and frequently another such structure, the appendix epididymidis (stalked hydatid) is attached to the head of the epididymis.
The ductus deferens is a cylindrical canal, about 40 cm in length, which begins at the tail of the epididymis, passes upwards parallel to the epididymis, becomes enclosed in the spermatic cord and passes with this through the inguinal canal. Then, after traversing the true pelvis, it reaches the back of the bladder, where it becomes enlarged to form the ampulla, and then unites with a seminal vesicle to form the ejaculatory duct, which opens into the prostatic portion of the urethra. Its wall is thick and muscular and its lumen quite small; consequently it is firm to the touch. In the interior of the ampulla the mucous membrane is thrown into numerous branching and anastomosing folds, associated with which there may be irregular outpouchings of the wall, the diverticula ampullae. The two ampullae become narrower below and converge.
The seminal vesicles are elongated, flattened bodies, which are attached, one on either side, to the lower end of the ampulla of the ductus deferens. Towards their blind upper ends they enlarge to form the body (corpus), but become more slender below. The surface of each is irregularly lobulated. Actually each seminal vesicle is a single, broad, contorted tube, with blind outpouchings of its walls, the various loops and outpouchings being firmly bound together by connective tissue. The blind end of the tube really lies some distance below what seems to be its upper end, this being merely one of the bends of the tube. The lumina of the vesicles are much wider than that of the ductus deferens, wider, indeed, than that of the ampulla, and the mucous membrane is thrown into strong folds.
The ejaculatory duct is a short narrow canal, weak in muscle tissue and lying entirely in the substance of the prostate. It is the prolongation of the ductus deferens beyond the point where it is joined by the seminal vesicle.
The skin of the scrotum passes without any boundary into that of the mons pubis, the perineum and the medial surface of the thigh. It is thin, distinctly pigmented and darker than the neighbouring skin; it possesses large sebaceous glands, a few strong hairs and a distinct median raphe, which corresponds to the septum within. This is a partition which separates the two testes and spermatic cords and is formed of connective tissue, some fatty tissue and some smooth muscle fibres. Furthermore the skin of the scrotum possesses an extensive layer of smooth muscle fibres, the tunica dartos; the fibres are arranged in a network.
Beneath the dartos is the cremasteric fascia, which is continued downwards from the superficial abdominal fascia over the Cremaster muscle and follows this to the scrotum. The muscle is an extension of the Obliquus abdominis internus and runs in scattered, at first longitudinal and parallel, bundles on the surface of the spermatic cord, but in the scrotum the bundles take oblique and transverse courses. They lie directly upon the fascial membrane, the tunica vaginalis communis, which is a continuation of the fascia transversalis of the abdomen and is so called because it forms a common sheath for the spermatic cord and the testis. The tunica vaginalis propria is the inner tunic of the testis. There are thus in the scrotum the following layers: the skin with the tunica dartos, the cremasteric fascia, the Cremaster muscle, the tunica vaginalis communis and the tunica vaginalis propria.
The spermatic cord (funiculus spermaticus) is a roundish cord about the thickness of the little finger and 10-12 cm in length. It extends from the inguinal canal to the upper end and posterior margin of the testis and contains as its chief constituents the ductus deferens behind and the testicular vessels in front, the veins that it contains forming a wide-meshed network, the pampiniform plexus. In addition it contains the deferential artery and vein, and the lymph vessels and nerves of the testis group themselves in the anterior and lateral parts of the spermatic cord, those of the ductus deferens in the posterior and medial parts. Furthermore there is in the cord the rudiment of the vaginal process, and in its lower portion the paradidymis; also smooth muscle fibres, the Cremaster internus. The coverings of the cord are a rather loose connective tissue, poor in fat, the cremasteric fascia, the Cremaster externus and the tunica vaginalis communis.
The male urethra, which is about 20 cm in length, consists of a prostatic portion, a membranous portion and a cavernous portion. The first of these lies in the prostate, which is really its thickened wall, its lumen transversing the gland from base to apex. It shows a longitudinal fold on its posterior wall, the urethral crest, the highest part of which is termed the colliculus seminalis. Upon its apex is the opening of the prostatic utriculus (uterus masculinus) and laterally those of the ejaculatory ducts (see also here). The membranous portion is about 1 cm in length and runs almost perpendicularly through the musculature of the urogenital trigone.
On either side of the posterior part of the membranous portion there is a roundish gland, the bulbourethral (Cowper's) gland, about the size of a pea and imbedded in the fibres of the Transversus perinei. Its duct is very thin, but rather long (4-5 cm), and runs forwards and downwards through the bulb of the urethra to open into the urethra at the beginning of its cavernous portion.
The cavernous portion is much the longest part of the male urethra and its walls are the corpus cavernosum urethrae. In its proximal portion it is convex backwards, then follows a portion below the symphysis which is concave upwards, the concavity being quite independent of the position of the penis (pars cavernosa fixa), and finally there is a portion in the pendulous part of the penis (pars pendula). Consequently in the lax penis the urethra shows an S-shaped curve, but in the erect organ the lower curve is straightened out, only the upper one remaining. The caliber of the cavernous portion is fairly uniform, except for an enlargement close to the external orifice. This enlargement is termed the fossa navicularis (Morgagni) and on its dorsal wall it has a semilunar fold, the valvula fossae navicularis (lacuna magna).
The penis is an almost cylindrical body, which is fastened by its root (radix) to the pubic bones, its principal portion, the body (corpus), hanging downwards when in a lax condition. The free thickened end is formed by the glans. It has a broader upper and anterior or dorsal surface and a somewhat smaller urethral surface, below and behind.
The chief constituents of the penis are the erectile corpora cavernosa penis, which are cylindrical bodies, tapering to a point anteriorly and posteriorly. They are fused together throughout the greater part of their extent. They take their origin from the medial borders of the inferior rami of the ischia by more slender flattened portions, the crura penis. In front of the lower part of the symphysis the two crura come together and their medial surfaces fuse to form the septum of the penis (see here).
The pointed anterior ends of the two corpora cavernosa penis project under the corona of the glans. Each corpus has a very firm and thick covering of connective tissue, the tunica albuginea, and in the body of the penis, where the corpora are fused, it forms the incomplete septum penis.
The third, more slender, but longer, erectile body in the penis is the corpus cavernosum urethrae, a distinctly flattened cylindrical structure, enlarged posteriorly to form the bulb and anteriorly to form the glans. It forms the wall of the cavernous portion of the urethra. The bulb is somewhat pyriform in shape and shows a furrow or sulcus which separates two hemispheres, more distinctly separated in the interior by a septum.
The glans penis has the form of a short, broad oblique cone, with a rounded tip. Its convex dorsal surface is longer than the ventral one, which has a shallow groove. The base of the glans is excavated to receive the anterior ends of the corpora cavernosa penis and its free projecting border is termed the corona, the region just behind this being the neck (collum). A septum extends from the albuginea upwards to the urethra.
The three corpora cavernosa are enclosed by a common, rather dense, connective tissue investment, which extends as far as the neck and is termed the fascia penis. It also encloses the dorsal vessels of the penis. At the neck of the glans the skin forms a strong fold, of greater or less extent, the prepuce. The skin covering the glans is very much thinner than usual, without hairs and with only occasional sebaceous glands; at the neck it is reflected forward so as to again cover the glans to a greater or less extent, and it then bends back upon itself to become continuous with the skin over the body of the penis. There is thus formed between the prepuce and the glans the preputial sack. The inner layer of the prepuce is bound to the glans by a frenulum, which is attached in the groove on the under surface of the glans.
The ovary has two surfaces, a medial surface turned toward the tuba uterina and largely covered by it and a lateral surface in contact with the wall of the true pelvis. They are separated by rounded borders, of which the free border (margo liber) is more convex and broader and looks backward and medially. The mesovarial border, along which the mesovarium is attached, is straighter and looks forward and laterally; it bears the hilus for the entrance and exit of vessels and nerves. The upper, strongly rounded tubar extremity is directed towards the infundibulum of the tuba uterina and the lower uterine extremity is fastened to the uterus by the ligamentum ovarii proprium (ovarian ligament), which passes to the fundus of the uterus between the two layers of the broad ligament. The tubar extremity is fastened to the infundibulum of the tuba by the fimbria ovarica and also to the pelvis by a connective tissue band containing muscle fibres and the ovarian vessels and nerves, the suspensory ligament of the ovary.
The ovary lies on the posterior layer of the broad ligament, the epithelium of which is continuous with the germinal epithelium of the ovary. Two layers may be seen in the ovary, a medullary and a cortical layer; the latter covers the entire surface except at the hilus and is characterized by containing the ovarian (Graafian) follicles (folliculi vesiculosi) or the corpora lutea formed from them.
The tuba uterina (Falloppian tube) is a paired, muscular tube, 10-15 cm in length, which occupies the upper edge of the broad ligament and connects the ovary to the uterus, although its union with the ovary is only indirect. It begins at the ovary by a round orifice that opens directly into the body cavity, the ostium abdominale, situated at the bottom of a funnel-like part of the tube, the infundibulum. This is much folded on its inner surface and ends in a number of fringe-like lobes, the fimbriae, one of which, the fimbria ovarica, extends to the tubar extremity of the ovary.
The portion of the tuba following on the infundibulum is the ampulla, which is broader than the portion nearer the uterus and has strong folds in its interior. It bends sharply around the tubar extremity of the ovary and then runs almost vertically, parallel and close to the mesovarian border of the ovary, resting on the pelvic wall. It then bends almost at right angles into the greatly narrowed isthmus, which passes almost horizontally to the uterus. The final portion of the tuba is that which passes through the wall of the uterus, the uterine part, and this opens into the cavity of the uterus by the ostium uterinum. The mucous membrane of the tuba is raised into folds, which are high in the ampulla, lower in the isthmus.
The uterus is a thick-walled, muscular, hollow organ that has the shape of a flattened pear. It has two principal portions, a large, upper one, the body (corpus), and a smaller lower one, the cervix, the two being separated by a constriction, at which the uterus is bent in such a way that the body forms with the cervix an angle which is more or less marked according to the extent to which the uterus is filled. This angulation converts the vesico-uterine pouch into a mere cleft. The uppermost portion of the body that projects dome-like above the level of the tubae uterinae is termed the fundus. The anterior or vesical surface is less convex than the posterior, which is termed the intestinal surface; the borders are right and left. In the cervix two portions are distinguishable, a lower one which projects into the vagina, the vaginal portion, and an upper one above the vagina, the supravaginal portion. The latter is transversely elliptical in form, the former slightly conical. The very thick walls of the uterus enclose a relatively small cavity, which in the body is termed the cavity of the uterus and in the cervix the canal of the cervix. The two communicate by the internal os (orificium internum). The cavity of the uterus is merely a cleft, from before backwards, that is to say in the direction of the flattening of the uterus, but in the transverse direction it is more extensive. It has the form of an isosceles triangle, one angle of which is at the internal os and the other two at the ostia uterina of the tuba. The line between the two ostia is the shortest side of the triangle. The canal of the cervix on the other hand is almost cylindrical, though slightly enlarged at its middle; it begins at the internal os and opens into the vagina by the external os (orificium externum). Its mucous membrane is raised on both the anterior and posterior walls into a series of folds, the plicae palmatae. The thick, swollen lips of the external os form the vaginal portion; the anterior lip (labium anterius) is shorter and does not project so far as does the longer posterior lip (labium posterius).
The vagina is a rather wide, dilatable canal, which extends from the uterus to the external genitals. In the empty condition it is strongly flattened from before backward, so that its lumen in transverse section has the form of the letter H turned sidewise.
The anterior wall is shorter than the posterior wall, since the ax1s of the uterus is oblique to that of the vagina (anteversio uteri), and the vaginal portion of the uterus projects into the vagina in such a way that its two lips are of different lengths. The anterior wall of the vagina is attached to the base of the short anterior lip, the posterior to that of the longer posterior lip, so that the wall of the vagina is firmly united to that of the uterus and the vaginal mucous membrane passes directly into that of the uterine lips. There is thus formed a small, circular space between the uterine lips and the vaginal wall, the fornix vaginae; it is much deeper behind than at the sides or especially in front. On the anterior as well as the posterior wall there is a system of arched, transverse folds, the rugae, which form in the middle line of each wall a longitudinal ridge, the columna rugarum. The lower part of the anterior columna is especially prominent, this being due to the urethra, which bulges forward the vaginal wall as the urethral carina and is visible even in the vestibule. The mucous membrane of the vaginal portion of the uterus is entirely free from folds.
The bulbus vestibuli is an erectile body, homologous with the bulb of the corpus cavernosum urethrae of the male, and consists of two almost completely separated portions. They are situated one on either side of the orifice of the vagina and are elongated bodies, rounded and thickened posteriorly and flattened on the sides. Anteriorly they become smaller and are connected by a venous plexus, placed between the urethral and vaginal orifices. The two bulbi together form, therefore, a horse-shoe-shaped structure open posteriorly towards the orifice of the vagina.
In the region of the vestibule there are also the paired greater vestibular glands (glands of Bartholin). They open close to the lateral margins of the orifice of the vagina at about the level between their posterior and middle thirds, just at the junction of the skin of the vestibule with the mucous membrane of the vagina; when the hymen is present the openings lie in front of it.
The entrance to the vulva is a median cleft, the rima pudendi, bounded laterally by strong cutaneous folds, rich in fatty tissue, the labia majora, which are connected anteriorly and posteriorly by the low anterior and posterior commissures. Above the rima is the mons pubis, due to an accumulation of fatty tissue in the skin. The outer surfaces of the labia majora have the usual characters of the skin, contain numerous sebaceous glands and strong hairs; the inner surfaces are more like mucous membrane. The ligamenta teretia of the uterus end in their fatty tissue.
The labia minora are also cutaneous folds like the labia majora, but are as a rule much shorter, smaller and thinner; they are placed parallel to the labia majora and medial to them. Usually their greatest height is near their anterior ends; posteriorly they become much lower and lose themselves in the frenulum, in front of the posterior commissure. They are destitute of hairs and of fat tissue, but, on the other hand, they are richly supplied with sebaceous glands.
The area bounded by the labia minora is termed the vestibule. In its anterior portion is the clitoris, which in its position and structure resembles the penis of the male, but differs in being much smaller and in not being traversed by the urethra. It has two crura arising from the ischia, a body (corpus) and a glans, and contains two small elongated erectile bodies, the corpora cavernosa clitoridis. Only the slightly thickened, rounded, anterior end of the clitoris, the glans clitoridis, projects sufficiently into the vestibule that the labia minora can unite in front of the glans to form a praeputium clitoridis, while behind the glans they form a low transverse fold, the frenulum clitoridis.
Immediately behind and below the frenulum there is the external orifice of the urethra and on this follows, in the most posterior part of the vestibule, the orifice of the vagina. Associated with this in virgins is an usually semilunar membrane, the hymen, arising from the posterior wall of the vagina. After parturition has taken place it is represented by irregular, often notched, scarred lobes or warts, the carunculae hymenales (myrtiformes).
The Levator ani consists of two portions. The Pubo-coccygeus arises from the pelvic surface of the pubis, close to the symphysis, and passes to the rectum in the vicinity of the anus and to the anterior sacro-coccygeal ligament. The Ilio-coccygeus arises from the tendinous arch on the surface of the Obturator internus and is inserted into the coccyx and the ano-coccygeal ligament.
The Coccygeus arises from the spine of the ischium and passes, on the pelvic surface of the sacro-spinous ligament, to the lateral border of the lower part of the sacrum and coccyx.
The Sphincter ani externus encircles the lower end of the rectum, partly arising from the coccyx.
The Ischio-cavernosus arises together with the corpus cavernosum penis from the lower ramus of the ischium and is inserted into the corpus cavernosum and the dorsal fascia of the penis.
The Bulbo-cavernosus arises in the male from the under side of the bulb of the corpus cavernosum urethrae and inserts into the corpus cavernosum penis. In the female it surrounds the orifice of the vagina like a sphincter.
The Transversus perinei superficialis arises from the medial border of the ischial tuberosity; it unites in the middle line with the muscle of the other side and with the Bulbocavernosus.
The Transversus perinei profundus lies in the urogenital trigone. It arises from the medial border of the inferior ramus of the ischium and from the inferior fascia of the urogenital trigone. The muscles of the opposite sides meet in a median raphe.
The Sphincter urethrae membranaceae lies in the urogenital trigone and arises from the transverse ligament of the pelvis and from the inferior rami of the pubis. It surrounds the membranous portion of the urethra, with mostly circular fibres.
The muscles of the perineum, using that term in its widest sense, may be divided into
The first group is represented by the External sphincter ani, which is composed of striated muscle fibres in contrast with the smooth fibres of the rectal wall (see Figs. B71, B72). Its arcuate fibres surround the anal opening and lie in part close under the skin, uniting anteriorly with the Bulbocavernosus and posteriorly reaching the tip of the coccyx, from which some of its fibres take origin. This partly muscular and partly tendinous attachment to the coccyx is also termed the anococcygeal ligament. The deeper layers of the muscle pass gradually into the Levator ani (for this muscle and the musculature of the pelvic outlet see here).
The muscles of the external genitalia are the Ischiocavernosus and the Bulbocavernosus, for whose origin and insertion see here. The Ischiocavernosus is similar in form in both sexes, but is much more strongly developed in the male than in the female. The Bulbocavernosus on the other hand differs in the two sexes in its development, form and function: In the male it is through almost its entire length an unpaired muscle with a median raphe, lying on the perineal surface of the bulb of the corpus cavernosum of the urethra, and only at its anterior end dividing into two small diverging slips; it acts as a compressor of the urethra ("Detrusor urinae" and "Ejaculator seminis"). In the female, on the other hand, its fibres arch around the opening into the vagina, especially on its posterior and lateral surfaces, and it consequently acts as a sphincter of this opening ("Sphincter cunni"). This marked difference in the arrangement of the muscle in the two sexes depends upon the different form of the bulb of the corpus cavernosum of the male as compared with the bulbus vestibuli of the female.
(See also here.)
The closure of the pelvic outlet is effected principally by two muscular plates, the pelvic diaphragm and the urogenital diaphragm (trigone). These plates are composed of muscles and the fascias pertaining to them.
While the pelvic diaphragm (see below), perforated by the rectum and similar in structure in the two sexes, closes the posterior portion of the pelvic outlet, the anterior portion, that between the two pubic and ischial rami, is closed by the urogenital diaphragm. This extends backward to a fine tendinous line, the transverse septum of the perineum, formed from its fascial layers (see below). It is perforated by the membranous portion of the urethra in the male and by the urethra and vagina in the female. It is formed essentially by the Deep transverse perineal muscle and the sphincter of the membranous urethra, together with their two strong fascias, the superior and inferior fascia of the urogenital diaphragm, to which the muscles are rather firmly attached. The musculature is traversed by numerous vessels, especially veins; the bulbourethral gland in the male and the greater vestibular gland in the female are imbedded in the musculature. (Figs. B222, B223, B224.)
The pelvic diaphragm is formed by the Levator ani (see here) and the fascias covering its pelvic and perineal surfaces, the superior and inferior fascia of the pelvic diaphragm. It has the form of a shallow funnel, whose apex is perforated by the rectum; in this region the fibres of the External sphincter ani pass over into the Levatores ani. A fossa, the ischiorectal fossa, filled with soft fat and especially deep in the male, separates the diaphragm from the skin of the anal region.
In the human body there are two circulations, the so-called greater or systemic circulation and the lesser or pulmonary circulation. The heart furnishes the propulsive force for both circulations and consequently consists of two portions, the so-called right and left "hearts". Each portion consists of two chambers, a ventricle and an atrium, the chambers of opposite sides being separated by a septum (see below), while those of the same side communicate through atrio-ventricular openings (ostia venosa).
From the ventricles the blood is driven into the arteries, the blood stream in these being directed centrifugally. For the greater or systemic circulation the aorta carries the blood from the heart. It arises from the left ventricle and the blood flowing in it is rich in oxygen (so-called arterial blood). After many branchings the finest branches of the aortic system (arteries) pass over into capillaries, through whose thin walls oxygen is given off to the body tissues and carbon dioxide is taken from them, the blood thus becoming "venous". From the capillaries the finest branches of the veins arise and, after repeated unions to form larger and larger stems, the two venae cavae are formed and trough them the blood is returned to the heart, but to the right atrium. The direction of the blood stream in the veins is accordingly centripetal.
From the right atrium the venous blood passes into the right ventricle from which the pulmonary artery carries it to the lungs. Through the walls of the capillaries of the lungs the blood gives off its carbon dioxide and takes up oxygen from the inspired air, so becoming arterial, and it is then carried by the pulmonary veins into the left atrium, whence it passes through the left atrio-ventricular opening into the left ventricle. The lymphatic system seems to be an appendage of the veins of the systemic circulation, the flow of its contained fluid (lymph) being centripetal only. Its vessels absorb the fluid that has passed through the walls of the capillaries into the tissues and return it to the veins.
The heart (cor) is an almost conical, thick walled, muscular sack, whose upper, broader, fixed end is termed the base and its lower, freely moveable end the apex. The apex is directed forward and to the left and belongs to the left ventricle. The heart has two surfaces, distinctly separated, especially in the empty organ, except that they pass into one another at the left border. One of these surfaces 1s convex forwards and looks somewhat upwards; it lies behind the body of the sternum and the adjacent left costal cartilages and hence is termed the sterno-costal surface. The other surface looks backwards and downwards and is termed the diaphragmatic surface, since it rests. on the Diaphragm, principally upon its centrum tendineum. This surface is also convex, but a little less so than the sterno-costal.
Of the so-called borders of the heart only the right one really deserves the name and then only in hearts empty of blood. On the left side the convex sternocostal surface passes over into the also convex diaphragmatic surface without any line of demarcation.
Above the base of the heart lie the atria and the two arteries that arise from the ventricles; below it are the ventricles. It is indicated externally by a circular groove, interrupted in front, the coronary sulcus, in which lie the main stems of the vessels that nourish the heart. It lies nearer to the upper end of the heart than to the apex and contains four openings, two arterial and two venous. Two longitudinal grooves, the anterior and posterior longitudinal sulci (interventricular grooves), indicate on the anterior and posterior surfaces of the heart the separation lines between the two ventricles, and also contain the stems of the arteries that nourish the heart (see below). The two longitudinal sulci unite to the right near the apex of the heart in a notch {incisura apicis), which is not always distinct.
The wall of the heart consists of three layers; most externally is the visceral layer of the serous pericardium, termed the epicardium, beneath which there are, at least in adult hearts, extensive deposits of fat, especially in the sulci and in the neighbourhood of the apex. Where the fat tissue is wanting the epicardium rests on the second or middle layer, the myocardium. This is the actual heart musculature and forms by far the thickest layer of the heart wall; in the ventricle it is more than 7/10 of its thickness. The elements of the musculature arrange themselves in a highly complicated manner into bundles and layers; here only the essential features of the arrangement can be described. One of the most notable characteristics is that the musculature of the ventricles and atria are completely independent one of the other; the ventricles have their own musculature, and so also the atria. An exception to this rule is found only in a single special muscle hand, the so-called conducting system or atrioventricular bundle, which stands in connection with the innervation of the heart and extends without interruption from the atrial musculature to that of the ventricles (see here).
The greater portion of the musculature of the atria, as well as that of the ventricles takes its origin from connective tissue fiber-bundles which are arranged in rings around the atrio-ventricular openings. These fibrous rings take their origin from two firm cartilaginous plates one on each side of the root of the aorta; on section these are rounded-triangular and are therefore termed fibrous trigones (right and left). The fibre bundles that pass out from them and surround the atrio-ventricular openings are termed the fibrous rings (right and left); the right ring, which is elliptical in form, surrounds unbrokenly the right atrio-ventricular opening, the left one, on the contrary, is incomplete between the two fibrous trigones, the adjacent root of the aorta filling in the gap. The fibrous rings separate the musculatures of the ventricles and atria, since both arise from them, and at the same time they serve for the attachment of the atrio-ventricular valves.
The musculature of the atria consists essentially of two layers, a superficial and a deep; the former is common to both atria, the latter forms an independent layer for each atrium. The common superficial layer is not present throughout all the extent of the atria, but represented essentially by fibres that occur chiefly on the posterior surface of the heart, where they pass from the vicinity of one auricular appendix to that of the other and are consequently termed the horizontal interauricular fasciculus. In addition there are also superficial vertical muscle bundles on the atria. The layer is weakest on the auricles, which are otherwise rather rich in muscle.
The musculature of the ventricles is arranged like that of the atria in so far as in these also there is a superficial layer common to both chambers and a distinctly stronger layer, peculiar to each ventricle. The superficial fibres cross the deep ones almost at right angles; the two layers, however, are by no means sharply separated, there being frequent passages of fibres from one to the other. The superficial layer is a completely closed sheet, only a few millimeters in thickness, the fibres on the posterior surface of the ventricle having a more vertical direction than those on the anterior surface; the posterior fibres run obliquely downwards and to the right, the anterior downwards and to the left. Both converge towards the apex of the heart where they disappear, passing deeply and forming what is termed the vortex. They pass to the inner surface of the left ventricle, where they form in part the musculature of the ventricular septum and in part pass to the trabeculae (columnae) carneae (see here) and the papillary muscles.
The deep fibres of the right ventricle arise from the posterior part of the left fibrous ring, in the angle between the two rings, and from the posterior and right portions of the right ring. They are less vertical than the superficial fibres that cover them, being almost horizontal near the base of the heart. They form the main mass of the wall of the right ventricle, in which they have a rather complicated arrangement.
The deep fibres of the left ventricle form by far the strongest muscle mass of the entire heart. They arise from the anterior portion of the left fibrous ring, especially from the left fibrous trigone and partly also from the adjacent part of the right fibrous ring. Their course is not so steep as that of the superficial fibres. The muscle bundles pass from the anterior surface of the ventricle over its rounder border to the posterior surface, where they bend into the ventricular septum, some, however, passing to the anterior papillary muscle. Another group of bundles runs on the inner surface of those just described back over the rounded border of the heart to the posterior surface of the ventricle and terminate partly on the right fibrous trigone and partly in the posterior papillary muscle.
(For the conducting bundle see here.)
The atrio-ventricular valves are duplicatures of the endocardium, fastened by their bases to the fibrous rings of the atrio-ventricular openings. They are divided by more or less deep incisions into lobes or cusps, of which that of the left opening has two (bicuspid valve), that of the right three (tricuspid valve). Weaker incisions may produce an incomplete division of the individual cusps. The thread-like tendons of the papillary muscles, the chordae tendineae, are attached to the edges and under surfaces of the cusps. When open the cusps hang loosely in the cavity of the ventricle, resting on its wall; when closed the free edges of the cusps come together, forming a shallow, funnel-shaped groove on the atrial surface.
The right ventricle is almost conical, but since its left surface, that towards the left ventricle, is concave, its transverse section is semilunar. Its apex does not reach the apex of the heart: From the ventricle the right atrio-ventricular opening leads into the right atrium, the right arterial opening into the pulmonary artery. The former is on the base of the ventricle and has usually a three-cusped valve, the tricuspid valve, the smaller anterior cusp being anterior and somewhat to the right, while the other two larger ones are posterior and medial. The arterial opening lies in the anterior left portion of the base of the ventricle, close to the septum, and is at the summit of a conical prolongation of the ventricle, the conus arteriosus. This is limited by a weak muscle ridge in the interior of the ventricle, the supraventricular crest. At the arterial opening are three semilunar valves, one of which is anterior and others right and left.
The right atrium is a somewhat conical cavity whose slightly curved apex is formed by the right auricle (auricular appendix). It includes the actual atrium and the venous sinus (sinus of the venae cavae), which is separated from the atrium proper by a muscle ridge, the terminal crest, corresponding to a groove on the outer surface. The sinus receives from above the superior vena cava and from below the stronger inferior vena cava, the openings of these being opposite one another and separated by a prominence of the atrial wall, the intervenous tubercle (Lower's). At the opening of the inferior vena cava there is a semilunar valve, often broken through in the adult, the valve of the inferior vena cava (Eustachian), which is placed between the opening of the vein and the right atrio-ventricular opening. In addition, the veins of the heart wall open into the right atrium by the coronary sinus, whose opening is between the valve of the inferior vena cava and the right atrio-ventricular opening. Here also there is a thin semilunar valve, the valvula of the coronary sinus (Thebesian). The minute openings of the numerous smaller veins of the heart are in the region of the atrial septum and on the right wall.
The septum throughout an elongated or oval area remains destitute of muscle, forming a translucent area, the membranous portion of the septum. It marks the position of the foramen ovale, which remains open until birth and forms a slight depression, the fossa ovalis, on the lower part of the septum; it is surrounded, especially at its upper and anterior parts, by a well developed muscular thickening, the limbus of the fossa ovalis (Vieussenii).
The left atrium is irregularly cubical in form and on its anterior wall the left auricle (auricular appendix) forms a conical appendage. The right wall is formed by the atrial septum and in the lower one there is the left atrio-ventricular opening (ostium venosum sinistrum). The openings of the four pulmonary veins are so placed that the pair from each lung are close together, while the two pairs are some distance apart. Rarely the two veins of the same side unite to form a single vein. In contrast to what is seen in the right atrium, the wall of the septum is smooth, except for the usually inconspicuous remains of the sickle-shaped valve of the foramen ovale.
The left ventricle has the form of an oval, truncated above. Its thick walls are convex throughout, even in the region of the septum. On its base, which is directed posteriorly and to the right, the left atrio-ventricular and arterial openings lie close together. The former has a bicuspid (mitral) valve and lies to the left of and behind the latter. One cusp, the anterior, looks forward and to the right, the other, the posterior, backwards and to the left. The posterior one takes its origin from the fibrous ring, the anterior partly from this and partly from the posterior part of the root of the aorta. As a result the upper surface of the anterior cusp passes over directly into the inner surface of the aorta. Connected with the bicuspid valve are two large papillary muscles, very constant both in number and position. The left arterial opening, the aortic, lies anteriorly and to the right at the base of the heart, in front of the anterior cusp of the mitral valve and behind the root of the pulmonary artery. Of its three semilunar valves, one is to the right and one to the left as in the pulmonary set, but the third is posterior. They possess well-developed lunulae and strong nodules.
The inner lining of the heart, the endocardium, is a membrane which is thin in the ventricles and auricular appendices, but thicker elsewhere in the atria. It lines the entire cavity of the heart, including the muscular elevations on the walls of the ventricles and in the auricular appendices. The former are partly more or less elevated ridges, termed trabeculae (columnae) carneae, partly conical projections, the papillary muscles, from which the majority of the chordae tendineae (see above) pass to the atrio-ventricular valves. The muscle trabeculae of the auricular appendices are termed pectinate muscles; they are covered by thin endocardium, have a more regular arrangement than the trabeculae carneae of the ventricles and are of about the same height.
The Conducting System of the heart consists of a special muscle bundle, the only one that is common to both the atria and the ventricles, and it owes its name to the fact that it serves for the transmission of contraction stimuli from the atria to the ventricles. From its course it is also known as the atrioventricular bundle.
The starting point of the atrioventricular bundle is Tawara's node (atrioventricular nodule), an elliptical thickening of the musculature of the atrial septum, measuring 0.6 mm in its longest diameter. It lies on the right slope of the right fibrous trigone, near and below the opening of the coronary sinus and beneath the posterior cusp of the semilunar valves of the aorta. From it there arises a single tract, the crus commune, which passes for a short distance in the atrial septum to reach the lower posterior border of the membranous septum, where it divides into a right and a left limb. The two limbs straddle, as it were: the upper border of the muscular septum of the ventricle. The division is at an acute angle, so that the right limb passes to the right ventricle, lying in the same plane as the crus commune, while the left limb bends to the left, gradually separating from the crus commune. The right limb is a small, circumscribed, almost cylindrical muscle bundle that runs in the musculature of the ventricular septum at a slight depth, partly, indeed, close under the endocardium.
The left limb also lies in the ventricular septum, more superficially than the right limb, lying so close under the endocardium that in parts it may be seen through it. From its origin from the crus commune it curves slightly forward in the direction of the apex of the heart, and, after a short course between the posterior aortic semilunar valve and the upper border of the muscular septum of the ventricle, divides into an anterior and posterior bundle.
The former passes beneath the endocardium to the columnae carneae to the medial side of the anterior papillary muscle and with these to the base of the muscle; the posterior bundle, also running beneath the endocardium, continues the direction of the left limb and so reaches the base of the posterior papillary muscle.
In addition to these atrioventricular bundles there is also a sino-auricular system which serves as a conduction path for the heart. It takes its origin from the Keith-Flack node, much less definite in its outlines than is Tawara's node. It lies at the junction of the sinus venosus with the right atrium proper and therefore in the region of the sulcus terminalis, close to the root of the superior vena cava, in intimate relation to the cardiac muscle fibres in the wall of the vein. It has a length of about 1 cm and a breadth of 3-5 mm and lies close beneath the epicardium.
The pericardium is a fibrous sack lined by a serous membrane. The parietal layer of the serous membrane is so intimately associated with the fibrous pericardium that both are included in the term pericardium, while the visceral layer which covers the heart and the parts of the great vessels that are within the pericardium is termed the epicardium.
The pericardium has a conical form (see here). Its base looks downwards and rests on the Diaphragm, to whose central tendon it is firmly united; it also rests on the muscular left dome of the Diaphragm but has no intimate connection with it. The apex looks upwards and is attached to the aorta at the junction of its ascending portion with the arch, so that the whole of the ascending aorta lies inside the pericardium. In addition the pericardium surrounds the pulmonary artery up to its division and the short portion of the inferior vena cava that is above the Diaphragm. A longer portion of the superior vena cava is included, namely, all of it that lies below the opening of the vena azygos (see here). However the boundary of the pericardium passes obliquely over the superior vena cava, so that more of the anterior than the posterior surface of the vein is covered by epicardium. The left pulmonary veins have only a short course within the pericardium, the right veins a longer one. The ligamentum arteriosum (Botalli) lies outside the pericardium, but produces an elevation upon its inner surface.
At the passage through the pericardium of the great vessels the fibrous layer of the membrane fuses with their walls, while the serous layer is reflected over the vessels as the visceral layer or epicardium. This reflexion of the parietal into the visceral layer takes place only at two regions and not at each of the eight vessels that pass through the pericardium. The two arterial trunks, which are united by connective tissue, have a common epicardial sheath and, in a similar manner, the parietal layer is reflected as epicardium upon the posterior wall of the atrium and the venous stems connected with it. Thus there is formed a transverse space, bounded in front by the arterial trunks and behind by the left pulmonary veins and the vena cava superior. This is the transverse sinus of the pericardium. In the adult it will give passage to 2 (-3) fingers. Between the atria and the terminations of the various veins, for instance between the left atrium and the left pulmonary veins, there are pockets which are sometimes deep, but blind, that between the inferior vena cava and the lower left pulmonary vein (the so-called oblique sinus) being the deepest.
The manner in which the parietal and visceral layers of the pericardium are reflected is as follows: The arterial reflexion has already been described, both arterial trunks being included in a common epicardial sheath, which bounds the transverse sinus anteriorly. More complicated is the reflexion upon the six venous trunks; to begin with the superior vena cava, which lies to the right of the transverse sinus, the line of reflexion passes from it at first transversely, forming the lower boundary of the transverse sinus, to the superior left pulmonary vein; there follows then an acute angled pocket, open to the left, at whose lower boundary the reflexion upon the inferior left pulmonary vein occurs; from here the line of reflexion, bounding the large pocket between the inferior vena cava and the inferior left pulmonary vein (see above), passes back parallel to the lower boundary of the transverse sinus to where the superior vena cava pierces the pericardium; it then runs almost vertically downwards, in this part of its course surrounding first both right pulmonary veins and then the inferior vena cava.
The form of the pericardium is that of a scalene triangle. From the base, adherent to the diaphragm, the shorter right side passes almost vertically upwards to the apex, while the longer, left side runs obliquely. The anterior surface of the pericardium lies behind the sternum and the costal cartilages and is fastened to these partly by loose connective tissue and partly by stronger bundles, the sterno-pericardial ligaments. A considerable portion of the anterior surface of the pericardium is covered by the thymus in the child; in the adult occasionally a much smaller portion is covered by the remains of the gland. The lateral surfaces of the pericardium are covered by the pericardial pleurae united to them by epi-pericardial connective tissue, which is often fatty, and between these portions of the parietal pleura and the pericardium the phrenic nerve, accompanied by the pericardiaco-phrenic vessels, passes downward to the diaphragm.
The circulation in the fetus differs from that of the adult in that the lesser or pulmonary circulation is still almost entirely wanting, the placental circulation taking its place. The two halves of the heart are in communication by an opening in the atrial septum, the foramen ovale.
The placenta, united to the wall of the uterus, is connected with the fetus by the umbilical cord, which contains two umbilical arteries and an umbilical vein. The umbilical arteries are identical with those of the same name in the adult but are so large that they appear to be almost direct continuations of the fetal aorta; they contain blood relatively poor in oxygen, since the fetal arteries do not contain any really "arterial" blood, but an almost mixed blood. In the placenta this blood is arterialized and is returned by the umbilical vein to the body of the fetus; here for the most part it passes through the liver by way of the later portal vein but partly goes directly into the inferior vena cava by the ductus venosus (Arantii), there becoming mixed with venous blood. Other venous blood is poured into the right atrium from the superior vena cava and the cardiac veins; the decidedly mixed blood thus produced can pass on by one of two routes.
A valve, that gradually becomes more and more insufficient towards the close of fetal life, the valvula venae cavae (Eustachian valve), incompletely prevents blood flowing from the right atrium into the right ventricle, but what does reach that cavity continues on into the pulmonary artery. This has a large communication, the ductus arteriosus ( Botalli), with the fetal aorta, so that all the blood in the pulmonary artery passes into the aorta, since the branches of the artery in the lungs are hardly capable of transmitting blood during the collapsed condition of the organs.
Only at birth, when the first breath draws air into the lungs and at the same time widens the branches of the pulmonary artery, does the lesser circulation become active; the foramen ovale of the atrial septum is closed by the valvula of the foramen; the communication between the two sides of the heart is thus closed; and the lumen of the ductus arteriosus becomes obliterated.
The arteries of the heart are the two coronary arteries, which take their origin from the right and left sinuses of the aorta.
Almost all the veins of the heart open into a large, but short common stem, the coronary sinus, which occupies the posterior part of the coronary groove and opens into the right atrium. The principal affluents are:
(For the posterior rami of the cervical nerves, see here.)
The cervical plexus is formed by the union of the ventral roots of the first to the fourth cervical nerves (C1-C4) (Fig. C12). Its branches are:
(For the Deep Veins, see here.)
The subclavian artery arises on the right side from the innominate artery, on the left directly from the aortic arch. It passes at first upwards behind the sterno-clavicular joint without giving off any large branches and, in the neck, forms an arch, strongly convex upwards, in which lies the dome of the pleura. It then runs behind the insertion of the Scalenus anterior to the subclavian groove on the first rib and over this to behind the clavicle. Its branches arise chiefly from the portion medial to the Scalenus, only the transversa colli arising from the lateral portion. Fig. C8, C9, C10, C11, C13, C18.
The branches of the subclavian, frequently inconstant, have a tendency to arise opposite one another or to branch from a common trunk; the ascending limb of the arch, much longer on the left than on the right, gives off no branches. The branches are the following:
(For the superficial veins of the neck, see here.)
The axillary vein is formed by the union of the two brachial veins and runs through the axilla, medial to and in front of the axillary artery, to open into the subclavian vein (see here) behind the Subclavius. Fig. C13, C14, C15 (not labelled), C18, C19. Its roots are:
The axillary artery is the direct continuation of the subclavian and at the lower end of the axilla is directly continued into the brachial artery. Fig. C10, C11, C13, C14, C15, C16, C17, C26, C33, C34. Its branches are:
The thoracic aorta is the portion of the aorta above the diaphragm and may be divided into three portions: I. the ascending aorta, II. the aortic arch and III. the descending aorta, which passes at the diaphragm directly into the abdominal aorta.
The internal mammary artery arises from the concavity of the subclavian (see here), almost opposite the vertebral artery which runs upwards towards the head, while the internal mammary runs downwards. At first it lies behind the subclavian vein and the sterno-clavicular joint and then passes through the anterior part of the upper aperture of the thorax and comes to lie on the posterior surface of the costal cartilages and the internal intercostal muscles. It runs downwards parallel to the lateral border of the sternum to what is termed Larrey's cleft of the diaphragm, to divide there into its two terminal branches. Posteriorly it lies partly directly on the costal pleura, partly on the Transversus thoracis. Its branches are:
The internal mammary vein corresponds in its course to the artery and the majority of its branches. It lies closely medial to the artery, and is usually a single stem on either side of the body, although at its origin on the diaphragm its branches are doubled companion veins. It opens usually into the left innominate vein. Fig. C21.
(See also here.)
The thoracic duct (see here), the chief lymphatic stem of the body, arises from the somewhat inconstant cisterna (receptaculum) chyli in front of the first lumbar vertebra. It passes upwards at first behind and then to the right of the descending aorta, between it and the v. azygos and in front of the right intercostal arteries. Fig. C22, C116, C356, (C359).
The twelve intercostal nerves, the last of which is below the twelfth rib, lie about midway in the intercostal spaces and between the two layers of muscles. They are the anterior rami of the twelve thoracic spinal nerves and do not form any plexus. Fig. C18, C22.
The anterior ramus of the first thoracic nerve forms only a small part of the first intercostal nerve, which is small in accordance with the narrowness of the first intercostal space; for the most part it unites with the anterior ramus of the eighth cervical nerve to take part in the formation of the brachial plexus (cf. Fig. C19). Fig. C12.
The intercostal nerves give off two series of cutaneous nerves. There is a strong series, the lateral cutaneous branches, in the axillary line, emerging between the serrations of the Serratus anterior and dividing each into an anterior and a posterior branch; the weaker, anterior cutaneous branches emerge with the perforating branches of the internal mammary artery. Fig. C14, C16, C17.
Each spinal nerve is a mixed nerve, formed from anterior motor and posterior sensory roots (see here). After a short course it divides into an anterior (ventral) and a posterior (dorsal) ramus, both of which contain both motor and sensory fibres. Except in the 2-3 upper cervical nerves the anterior ramus is much larger than the posterior, and in the cervical, lumbar and sacral regions they form by union with neighboring ventral branches, the cervical, brachial, lumbar, and sacral plexuses. The ventral rami of the thoracic nerves form the intercostal nerves, only the first taking part in the formation of the brachial plexus. The ventral rami also send rami communicantes to the adjacent sympathetic ganglia, these, however, being constant in the cervical nerves.
The dorsal rami, with the exceptions mentioned above, are much weaker than the ventral and do not form plexuses. They penetrate the dorsal musculature, dividing into medial and lateral branches which supply the musculature and may reach the skin by their terminal branches. In the neck and upper part of the back the medial cutaneous branch is the stronger, the lateral frequently not reaching the skin. In the lower part of the back and in the lumbar region the lateral branch is the stronger. The dorsal rami of the sacral nerves are quite weak and almost purely sensory. Fig. C23, C25.
The following receive special names (see here).
(See also here and here). During its course through the foramina of the transverse processes of the cervical vertebrae (Fig. C11) the vertebral artery gives off spinal branches to the spinal cord, as well as muscular branches to the muscles of the back of the neck, the branches from the upper part of the artery being the stronger. From the transverse foramen of the atlas it bends in an arch over the posterior arch of the atlas, pierces the posterior atlanto-occipital membrane and enters the foramen magnum (see here). Fig. C11, C25.
(cf. here.)
The infraclavicular portion of the brachial plexus consists of three cords which surround the upper part of the brachial artery and are named according to their relations to it (Fig. C26).
The axillary artery is the direct continuation of the subclavian and at the base of the axilla it passes directly into the brachial artery. Fig. C10, C11, C13, C15, C27, C33, C34. Its branches are:
In addition to the posterior supraclavicular nerves (see here, Fig. C29, C31) supplying a part of the skin of the shoulder, there are the following:
The brachial artery is the direct continuation of the axillary (see here) and is accompanied by two brachial veins and the median nerve. It passes downwards beneath the brachial fascia in the medial bicipital groove to the cubital fossa, where it lies upon the tendon of insertion of the Brachialis, covered by the lacertus fibrosus. It divides into two terminal branches, the radial and ulnar arteries. Fig. C33, C34, C35, C36, C37, C38, C39. Its branches are:
arises from the lateral cord of the brachial plexus, traverses as a rule the Coraco-brachialis, giving branches to it, and comes to lie between the Biceps and Brachialis. It supplies both these muscles and becomes superficial as the lateral antebrachial cutaneous nerve (see here) at the radial border of the tendon of insertion of the Biceps. Fig. C29, C30, C33, C34.
The radial (musculo-spiral) nerve is a mixed nerve and the largest of the brachial nerves. It arises from the posterior cord of the brachial plexus and lies at first behind the brachial artery. It then passes, in company with the deep brachial artery, between the long and medial heads of the Triceps and later between the medial and lateral heads, close to the bone, in the groove for the radial (musculo-spiral) nerve, on the posterior surface of the humerus. It then follows the course of the groove and, piercing the lateral intermuscular septum in company with the volar branch of the radial collateral artery (see here), it comes to lie in the groove between the Brachialis and the Brachia-radialis, where it divides into its two terminal branches. Fig. C33, C34, C35, C36, C37, C38, C39, C41. Its branches are:
arises at the bend of the elbow by the division of the brachial artery (see here), being its weaker terminal branch. It runs at first between the lacertus fibrosus and the tendon of the Biceps, then passes to the ulnar side of the superficial radial nerve under cover of the Brachio-radialis and runs downwards in the groove between this and the forearm flexors, first in front of the tendon of the Pronator teres and then between the Brachioradialis and the Flexor carpi radialis. It rests for some distance on the Flexor pollicis longus and for a short distance on the Pronator quadratus and in the lower third of the forearm it is covered only by the antebrachial fascia and lies accordingly quite superficially in front of (volar to) the styloid process of the radius. Below this it bends under the tendons of the Abductor pollicis longus and the Extensor pollicis brevis to the dorsum of the hand, traversing the radial foveola (tabatière), and there passes between the two heads of the first dorsal Interosseous muscle to the volar surface of the hand to form the deep volar arch. Fig. C37, C38, C39, C40, C41, C47, C48, C49, C50. Its branches are:
Continued here.
arises in front of the lower part of the axillary artery by the union of two branches which come from the medial and lateral cords of the brachial plexus. In the upper arm it lies at first on the lateral side of the brachial artery, but crosses in front of it in the lower third of the upper arm and so comes to lie medial to the artery. Along with it it passes through the bend of the elbow, covered by the lacertus fibrosus, accompanies the upper part of the ulnar artery for a short distance, passes between the ulnar and humeral heads of the Pronator teres, crosses over the ulnar artery and runs down the forearm between the superficial and deep layers of flexors. With the tendons of these it passes through the carpal canal into the palm of the hand, where its terminal branches are given off. Fig. C26, C33, C34, C37, C38, C39, C40, C41, C49. It is a strong, mixed nerve. It gives off no branches in the upper arm; its branchings begin in the cubital fossa and are:
arises in the cubital fossa as the stronger terminal branch of the brachial artery (see here). It curves gradually toward the ulnar side of the volar surface of the forearm, being situated on the origin of the Flexor digitorum profundus and behind the median nerve and the superficial flexors. It comes to lie on the radial side of the ulnar nerve, but in contrast to the radial artery, it remains covered by the Flexor digitorum sublimis and the Flexor carpi ulnaris until the lower fourth of the forearm, where it becomes visible between the tendons of these two muscles, close beside the ulnar nerve. With this it runs over the radial surface of the pisiform bone between the volar and transverse carpal ligaments, and so, covered at first by the Palmaris brevis, to the palm of the hand, where it is the chief constituent of the superficial volar arch. Fig. C37, C38, C39, C40, C44, C49, C50. Its branches are:
is formed from the medial cord of the brachial plexus and is a mixed nerve. It lies at first on the medial side of the brachial artery but as it descends the arm it inclines more and more toward the medial intermuscular septum, in which it comes to lie superficially or imbedded and is accompanied by the superior ulnar collateral artery. The nerve then passes between the medial epicondyle and the olecranon, and then bends deeply and volarly, passing between the Flexor carpi ulnaris and the Flexor digitorum profundus. At this level it begins to give off its branches, supplying the former muscle and part (ulnar half) of the latter. It comes to lie close to the ulnar side of the ulnar artery (see here), runs down the forearm with this, and, passing close to the pisiform bone, enters the palm of the hand, after it has given off a branch for the dorsal surface. Fig. C26, C33, C34, C37, C38, C39, C40. Its branches are:
The deep veins of the upper extremity accompany the arteries as paired venae comites. They take origin in the deep and superficial volar venous arches and terminate with the brachial veins, from which the axillary vein is formed. They are connected by numerous anastomoses (venae intercapitulares, etc.) with the superficial veins (see here, Fig. C28, C29, C30) and during their course along with the arteries the members of each pair are frequently connected by transverse anastomoses.
is formed by the anastomosis of the terminal branch of the ulnar artery with the superficial volar branch of the radial. It is convex distally and lies between the palmar aponeurosis and the sheaths of the Flexor tendons, at about the middle of the length of the palm of the hand. From its convexity the common volar digital arteries II-IV arise; in the region of the finger webs these divide into proper arteries for the sides of the three middle fingers, the proper artery for the fifth digit arising independently from the ulnar artery and the three radial ones from the princeps pollicis. Fig. C49.
On its entrance into the palm of the hand the radial artery (see here) divides into the a. princeps pollicis and the chief branch to the deep arch.
The a. princeps pollicis divides between the thenar muscles into the proper volar radial digital artery for the thumb and a short stem, the volar digital artery I, which supplies the adjacent sides of the thumb and index finger; it represents a volar metacarpal artery I. Fig. C50.
The deep volar (palmar) arch is formed chiefly by the anastomosis of the terminal branch of the radial artery with the deep volar branch of the ulnar. It is situated more proximally than the superficial arch and is less convex, though longer, and it lies between the Interossei volares and the sheaths of the Flexor tendons and the Adductor pollicis. From it there arise, in addition to small branches to the volar carpal rete, the volar metacarpal arteries II-IV, which supply the Interossei and, in the region of the capitula of the metacarpal bones, anastomose with the common volar digital arteries. Fig. C50.
These come partly from the facial nerve, motor branches for the mimetic facial musculature, but the sensory nerves come from all three divisions of the Trigeminus, from the Vagus (n. auricularis, see here), from the cervical plexus and from the posterior branches of the cervical nerves.
The facial nerve, in its extracranial portion (see here), is a motor nerve. It leaves the skull through the stylo-mastoid foramen and runs in a gentle curve, concave upward, below the external auditory meatus between the lobes of the parotid gland, covered, however, by the main mass of the gland and divided into several anastomosing branches (the parotid plexus). At the anterior border of the gland it gives off its terminal branches to the muscles of the face. Fig. C51, C52, C53, C54, C55. Its branches are:
The following branches arise from the parotid plexus:
The common carotid artery on the left side arises directly from the arch of the aorta, on the right from the innominate artery, and runs up the neck in company with the internal jugular vein and the vagus nerve. It is covered at first by the Sterno-mastoideus, later appearing at its anterior border in the carotid fossa, in which, placed rather superficially, it divides into its two terminal branches, the external and internal carotid. It has no other branches. Fig. C7, C8, C9, C10, C11, C15, C17, C18, C20, C55, C57, C58.
The external carotid artery runs upwards through the carotid fossa almost in the line of the common carotid, giving off large branches and diminishing rapidly in caliber. At first it is somewhat superficial, but higher up is covered by the posterior belly of the Digastricus and by the Stylo-hyoideus. Higher still it is covered by the parotid gland, as it runs along the posterior border of the ramus of the mandible up to the level of the neck of that bone. Fig. C8, C9, C13, C14, C15, C56, C57, C58. Its branches are:
runs beside the internal carotid artery in the wall of the cavernous sinus to the superior orbital fissure and divides on its entrance into the orbit (Fig. C50, C51, C52, C53, C114, C135) into
runs beside the internal carotid artery and the oculomotor nerve m the wall of the cavernous sinus (Fig. C60, C61, C62, C135, C138, C139) and through the superior orbital fissure into the orbit to supply the Obliquus superior. Fig. C60, C61.
runs beside the preceding with the internal carotid through the cavernous sinus (Fig. C60, C114, C135) and through the superior orbital fissure to the medial surface of the Rectus lateralis. Fig. C60, C61, C62, C135, C138, C139.
The ophthalmic artery is the only large branch given off by the internal carotid before it reaches the brain (see here). It passes through the optic foramen below the optic nerve and then inclines to the lateral side of the nerve, giving off its first branches. It then crosses above the optic nerve to the medial surface of the orbit and passes to the vicinity of the pulley for the Obliquus superior. Fig. C60, C61, C62, C63, C138. Its branches are:
runs beside the internal carotid artery and the nerves to the orbital muscles in the wall of the cavernous sinus, where it gives off a tentorial branch, and at the superior orbital fissure, lying superficially, it divides into three terminal branches. Fig. C60, C61, C68, C69, C70, C71, C135, C138, C139.
The ciliary ganglion is a flat, somewhat quadrangular structure about the size of a hemp seed, to whose posterior extremity three roots are attached; the slender long root from the naso-ciliary nerve, the strong short root from the oculo-motor and fine twigs forming the sympathetic root from the internal carotid plexus. From the anterior end of the ganglion the slender short ciliary nerves pass along the optic nerve to the eyeball, Fig. C61, C62, C114.
passes through the foramen rotundum into the pterygo-palatine fossa, where it gives off some branches and divides into its terminals. Fig. C66, C67, C68, C69, C70. Its branches are:
is a flat, triangular structure, situated in the pterygo-palatine fossa, medial to the maxillary nerve and close to the spheno-palatine foramen. It receives three roots:
The ganglion gives off the following branches.
(Cont. from here.)
The descending palatine artery gives off the small artery of the pterygoid canal (Vidian), which passes to the tuba auditiva and its surroundings and descends in the pterygo-palatine canal. It divides into the greater palatine artery to the hard palate and the lesser palatines to the soft palate. Fig. C66.
The spheno-palatine gives off the lateral-and medial posterior nasal arteries to the walls and septum of the nose. The posterior artery of the septum (naso-palatine) reaches the incisive canal. Fig. C64, C65, C66, C67.
contains the motor portio minor and is consequently a mixed nerve. It passes through the foramen ovale and immediately branches. Fig. C58, C59, C60, C61, C62, C63. Its branches are:
is situated on the medial surface of the mandibular nerve immediately below the foramen ovale. It is a small, flattened, plexiform body, which receives branches from the auriculo-temporal, internal pterygoid and chorda tympani and, in addition, sympathetic fibres from the meningeal plexus and the lesser superficial petrosal nerve from the glosso-pharyngeal (see here). From the ganglion are given off,
The facial nerve, intracranial portion, runs in the facial canal of the temporal bone, receives the n. intermedius while still in the skull in the vicinity of the internal auditory opening (Fig. C69), forms the geniculate ganglion at the knee of the facial canal and gives off from this the greater superficial petrosal nerve. This passes through the hiatus of the facial canal, through the foramen lacerum, and through the pterygoid canal, to pass to the spheno-palatine ganglion. Fig. C66, C67, C71 (see here). The facial nerve also gives off branches to the tympanic plexus (see below) and to the Stapedius muscle and just above the stylo-mastoid foramen the chorda tympani (actually the n. intermedius) is given off to join the lingual nerve (see here). The chorda passes through the bone to the tympanic cavity, across this between the malleus and incus, and leaves it by the petro-tympanic fissure. Fig. C68, C69, C71, C73, C114 (see also here).
The ascending pharyngeal artery arises from posterior wall of the external carotid near its beginning (Fig. C57) and passes upwards on the lateral wall of the pharynx, to which it gives pharyngeal branches. It terminates at the base of the skull in the inferior tympanic (accompanying the tympanic nerve) and the posterior meningeal (passing through the jugular foramen to the dura mater). Fig. C72.
The glossopharyngeal nerve, the ninth cranial nerve, is a mixed nerve. It passes through the jugular foramen with the vagus and accessorius, forming the small superior ganglion, receives fibres from the superior sympathetic ganglion and forms the petrosal ganglion. Then it passes between the two carotid arteries and applies itself to the medial surface of the Stylopharyngeus, with which it runs to the pharynx. Fig. C72, C114. Its branches are:
The (Spinal) Accessory Nerve also passes through the jugular foramen and immediately below this divides into the internal branch, that joins the vagus (Fig. C72), and the external branch. This passes in front of the internal jugular vein to the medial surface of the Sterno-mastoideus, which it penetrates above its middle, giving off muscular branches. It leaves the muscle at its lateral border and passes obliquely downwards and laterally through the supraclavicular fossa, uniting with branches of the cervical plexus, to the anterior surface of the Trapezius, which it supplies. Fig. C8, C9, C10, C13, C23, C25.
The Hypoglossal Nerve leaves the skull through the hypoglossal canal and lies at first medial to and behind the vagus nerve and the internal jugular vein. It then curves forwards and laterally on the lateral side of the internal and external carotids, medial to the Digastricus and Stylo-hyoideus, to reach the submaxillary region. It then crosses the lateral surface of the Hyo-glossus, which separates it from the lingual artery, and passes to the tongue. Fig. C9, C10, C13, C14, C15, C75, C114. In addition to connections with the vagus and sympathetic it gives off the following branches.
(see also Fig. C114 and C117, and here.)
forms in the jugular foramen a jugular ganglion and receives the internal branch of the accessory nerve. Below the foramen it forms the larger, elongated ganglion nodosum and then runs downwards with the internal carotid artery (lower down with the common carotid) and the internal jugular vein, lying between the two and at first behind, but later in front of them. It passes into the thorax, the left vagus passing in front of the arch of the aorta and the right over the right subclavian artery; they then run along the two bronchi to the hilus of the lung, and then pass through the diaphragm with the oesophagus to the stomach (and intestine). Fig. C10, C13, C18, C20, C72, C114, C115, C116, C117.
The principal branches of the vagus are:
arises from the superior thyreoid (see here) and passes to the larynx between the greater cornu of the hyoid bone and the upper border of the thyreoid cartilage. It gives branches to the Sterno-mastoideus and the neighboring muscles of the tongue, and also the long crico-thyreoid branch to the Crico-thyreoid muscle and ligament. The main stem of the artery goes with the superior laryngeal nerve through the hyo-thyreoid membrane to the interior of the larynx. Fig. C9, C10, C13, C14, C15, C74.
from the external carotid (see here) runs at first horizontally immediately above the greater cornu of the hyoid bone, separated from the hypoglossal nerve by the Hyo-glossus. It then runs rather steeply upwards, at first between the Hyo-glossus and Genio-glossus and then between the latter and the Longitudinalis inferior as far as the tip of the tongue. Fig. C9, C64, C75.
Its branches are:
begins at the aortic opening of the diaphragm, as the direct continuation of the thoracic aorta. It lies on the anterior surfaces of the lumbar vertebrae, almost in the median line and to the left of the inferior vena cava. In front of the fourth lumbar vertebra it divides into its terminal branches, the two common iliac arteries. Fig. B109, B110, C76, C77, C79, C80, C82, C83. Its branches are visceral and parietal.
These are the largest and most important branches of the abdominal aorta and may be divided into the unpaired and the paired branches.
The continuation of the abdominal aorta, beyond its division into the two terminal common iliac arteries (see here), is the middle sacral artery. This arises at the point of bifurcation of the abdominal aorta and continues in its direction, running downwards in the median line over the body of the fifth lumbar vertebra and the pelvic surface of the sacrum. In front of the tip of the coccyx it terminates in a vascular knot, the glomus coccygeum. In addition to numerous small branches to the neighboring muscles and bones (transverse branches on the sacrum that anastomose with the lateral sacral arteries) it gives off the paired lowest lumbar arteries, which, much weaker than the fourth pair, run over the body of the fifth lumbar vertebra to supply the Psoas and Iliacus, anastomosing with the iliolumbars. Fig. C80, C82, C88.
The portal vein is a short and large venous trunk that is formed by the union of the superior mesenteric and splenic (lienal) veins, behind the neck of the pancreas. It continues in the region of the pancreatic notch the course of the former, enters the hepatoduodenal ligament at the upper border of the pancreas, lying behind the hepatic artery and the bile duct (Fig. B81), and divides into two branches which enter the porta of the liver. It is the afferent vessel of the hepatic circulation and carries to the liver the venous blood from all the unpaired organs of the abdomen; i.e. from the digestive tract, including the liver and pancreas, and from the spleen, since the inferior mesenteric vein opens into the splenic (lienal) vein or more rarely into the superior mesenteric; within the liver substance the capillaries of the hepatic artery also pass into the roots of the portal vein.
(See here for the pelvic part).
The inferior vena cava is formed by the confluence of the two common iliac veins in front of the fibrocartilage between the 4th and 5th lumbar vertebrae. It runs upwards on the right side of the abdominal aorta and in close relation to it, but before it passes through the diaphragm it comes to lie in the fossa for the vena cava on the under surface of the liver and parts company with the aorta. In addition to its two roots it receives the upper four pairs of lumbar veins, the right internal spermatic, the two renal veins and, shortly before it passes through the diaphragm, the hepatic veins. Fig. B77, B77, B110, C80, C82, C83.
The lowest lumbar veins open into the middle sacral vein and this into the left common iliac; this passes over the middle sacral vessels, but behind the right common iliac artery. The left renal vein receives the left internal spermatic and crosses in front of the aorta. Fig. C82.
arises in front of the fibrocartilage between the fourth and fifth lumbar vertebrae by the union of the two common iliac veins and runs upwards close to and on the right of the abdominal aorta. Later it bends somewhat to the right towards the liver, joining its inferior surface in the fossa for the vena cava, and then, piercing the diaphragm (foramen venae cavae), it enters the thoracic cavity (pericardial cavity) and so reaches the heart. Fig. B076, B109, B110, C76, C80, C82, C83. Its tributaries are either parietal or visceral.
(Fig. C80, C81, C82, C83, C118)
The lumbar plexus is formed by the anastomoses of the anterior branches of the 1-4 lumbar nerves and lies partly behind the Psoas and partly between its bundles. In addition to muscular branches to the Quadratus lumborum and the Psoas it gives origin to the following nerves:
(Continued from here.)
The common iliac artery is a strong vessel resulting from the bifurcation of the abdominal aorta. Situated at first in front of the body of the (fourth and) fifth lumbar vertebra, it runs for about 5 or 6 cm along the medial border of the Psoas, being crossed by the ureter, and divides into its two terminal branches without giving off any other branches of even moderate size. Fig. C80, C82, C83, C88.
The external iliac vein begins in the lacuna vasorum as the direct continuation of the femoral vein. It passes upwards medial to and behind the femoral artery to form the common iliac vein (see here), anterior to the sacro-iliac articulation. Fig. C80, C82, C83, C84, C85. It usually receives only two tributaries, which may open together.
A short thick trunk that lies behind the artery of the same name and is formed from veins which correspond to the branches of the artery, although characterized by a tendency to form plexuses, a condition especially marked in the true pelvis. Fig. C80, C84, C85. Its tributaries run singly or doubly (gluteal veins) with the branches of the artery (Fig. C80, C83, C84, C101). The following frequently anastomosing plexuses open into the vein.
A rather weak plexus formed principally by the 3rd and 4th sacral nerves. It is closely associated with the sacral plexus (see here) and, like this, is situated in front of the origin of the Piriformis. Fig. C88. The following nerves arise from it.
By far the smallest nerve plexus in the body, is formed by the last sacral and the coccygeal nerve. It is closely associated with the pudendal plexus and is connected with the coccygeal sympathetic ganglion. Fig. C88. In addition to branches to the Coccygeus, only four or five anococcygeal nerves arise from the plexus, these passing to the skin behind the tip of the coccyx. Fig. C88, C89, C90.
The great saphenous vein, the largest superficial vein in the body, arises on the dorsum of the foot from the dorsal venous rete and from the medial end of the dorsal venous arch. It receives some veins from the plantar region and then passes up the medial surface of the lower leg and the thigh, inclining towards the anterior surface in the upper third of its course. It passes over the falciform border of the fascia lata and empties into the femoral vein. On its way it receives numerous branches, those of the thigh being the larger, and just before its termination it receives the superficial epigastric and superficial circumflex iliac veins and usually also the external pudendals. Fig. A312, C91, C92, C94, C108.
The small saphenous vein arises on the lateral side of the dorsum of the foot. It ascends behind the lateral malleolus on the posterior surface of the lower leg and, in the groove between the two heads of the Gastrocnemius, it pierces the fascia to open into the popliteal vein in the popliteal fossa. Before its termination it receives a vein from above, the femoro-popliteal, and by this and other anastomoses is brought into connection with the great saphenous. It is also connected with the deep veins of the lower leg by a strong branch. Fig. C91, C94, C108.
The cutaneous nerves of the leg come mainly from the lumbar plexus (the anterior surface of the thigh, and, by the saphenous nerve, the lower leg to the foot) and sacral plexus (posterior surface of the thigh, the lower leg and foot); only to a small extent from the pudendal plexus and from the posterior branches of the lumbar and sacral nerves.
The femoral artery begins behind the inguinal (Poupart's) ligament as the direct continuation of the external iliac artery (see here). It runs superficially through the ilio-pectineal fossa and the femoral trigone, covered by the fascia lata, at first lateral to and then in front of the femoral vein and medial to the femoral nerve. It then enters the adductor canal, covered by the Sartorius, and passes through the adductor hiatus into the popliteal fossa to become the popliteal artery. Fig. C95, C96, C97. Its branches are:
formed from the lumbar plexus (see here), passes with the Ilio-psoas through the lacuna musculorum, lying lateral to the artery and separated from it by the deep layer of the fascia lata (ilio-pectineal fascia). Below the inguinal (Poupart's) ligament it divides into:
Formed from the lumbar plexus (see here), passes through the obturator canal, giving branches to both the Obturator muscles. In the thigh it branches into:
The obturator artery, from the internal iliac (hypogastric) (see here), is relatively much weaker than the nerve. Like this it divides, after it has passed through the obturator canal, into an anterior and a posterior branch, which supply the Adductors. The posterior anastomoses with the medial femoral circumflex. Fig. C84, C96, C97.
The femoral vein is the continuation of the popliteal vein (see here). In the lower part of its course, in the Adductor canal, it lies behind the artery, but passes medially as it ascends and in the region of the fossa ovalis and below the inguinal ligament it is medial to the artery. It receives the deep femoral vein, the great saphenous (see here) and usually a number of small branches corresponding to the branches of the femoral artery. These last are double as is also the deep femoral, though this usually becomes single before its termination. Fig. C95, C96, C97.
The sacral plexus (Fig. C81) is a broad flat cord which passes through the great sciatic notch and divides into the following branches.
This is the direct continuation of the femoral artery (see here) and begins at the adductor hiatus. It ends in the popliteal canal, where it divides into its terminal branches. It runs through the middle of the popliteal fossa, resting on the femur and the posterior surface of the knee joint, and somewhat medial to the vein. It passes between the two heads of the Gastrocnemius, over the posterior surface of the Popliteus and under the popliteal arch of the Soleus, and then divides into the anterior and posterior tibial arteries. Fig. C100, C102, C103, C104, C105, C107. Its branches are:
(Cont. from here.)
A small network situated on the great trochanter of the femur, under cover of the Glutaeus maximus. It is formed by fine branches of both the gluteal arteries and of the deep branch of the medial circumflex femoral. Occasionally branches of other arteries, the lateral femoral circumflex, the first perforating, participate. Fig. C100, C101.
Follows the course of the popliteal artery through the popliteal fossa, lying behind and somewhat lateral to it. It is double in the lower part of its course, this double portion having origin from the doubled anterior and posterior tibial veins. Fig. C102, C103, C104.
(see here.)
The tibial nerve rises in the thigh by the division of the sciatic nerve. It passes vertically through the popliteal fossa, behind and lateral to the popliteal vessels. It enters the popliteal canal with them and runs on the lateral side of the posterior tibial artery, at first between the Soleus and the deep flexors, and then under the laciniate ligament behind the medial malleolus to the foot, where it divides into its terminal branches. Fig. C100, C102, C103, C104, C105. Its branches are:
(see here)
The posterior tibial artery rises in the popliteal canal, as the stronger terminal branch of the popliteal artery. It passes downwards with the tibial nerve (see above) between the Soleus and the deep Flexors (Tibialis posterior and Flexor digitorum), and, in the lower third of the leg, passes out from under the medial border of the Soleus and comes to lie beneath the fascia. It then runs behind the medial malleolus under the laciniate ligament to the sole of the foot, where it divides into its terminal branches, the medial and lateral plantar arteries (see here). Fig. C104, C105, C107, (C111, C112, C113). In addition to muscular branches and the nutrient artery to the tibia its branches are:
(see here)
Immediately after its origin from the popliteal artery passes between the tibia and fibula and runs downwards on the anterior surface of the interosseous membrane. It lies at first between the Tibialis anterior and the Extensor digitorum longus, and, lower down, between the Tibialis and the Extensor hallucis longus, accompanying the deep peroneal nerve. It passes under the cruciate ligament, resting on the bone and the capsule of the ankle joint, and on the dorsum of the foot is known as the dorsal pedal artery (see here). Fig. C105, C106, C110. In addition to muscular branches to the Extensors and in part to the Peronei, it gives off:
The common peroneal nerve runs from its origin (see here) along the lateral border of the popliteal fossa, that is to say along the Biceps femoris, to the head of the fibula. It curves forward around this, covered by the origin of the Peronaeus longus, and divides into its terminal branches. Fig. C100, C102, C106, C108. It gives off the following branches:
(see here)
The dorsal pedal artery is the direct continuation of the anterior tibial artery. It passes upon the dorsum of the foot between the tendons of the Extensor hallucis longus and the Extensor digitorum longus and, resting on the dorsal surfaces of the tarsal bones, takes a straight course to the first intermetatarsal space. Here it divides into its two terminal branches. Fig. C106, C110. Its branches are:
(See here)
The plantar arch is formed by the anastomosis of the lateral plantar (see here) with the deep plantar branch of the dorsal pedal. Occasionally the distal end of the medial plantar also takes part in the anastomosis (see here). It is convex forward and lies between the plantar Interossei and the oblique head of the Adductor hallucis. In addition to muscular branches it gives off four plantar metatarsal arteries, each of which divides into two plantar digitals. Fig. C113.
The medial plantar nerve arises below the medial malleolus by the division of the tibial nerve (see here) and, on entering the sole of the foot, lies medial to the terminal part of the posterior tibial artery. It then accompanies the medial plantar artery under cover of the Abductor hallucis, and runs between the Flexor digitorum brevis and the Quadratus plantae toward the toes. Fig. C111, C112, C113. In addition to small branches to the skin of the sole it gives off:
(see here.)
The lateral plantar nerve, the second terminal branch of the tibial nerve in the sole of the foot, accompanies the lateral plantar artery, lying on its medial side, and passes between the Flexor digitorum brevis and the Quadratus plantae. In the lateral plantar groove it divides into its terminal branches. Fig. C112, C113. In addition to small cutaneous branches to the skin of the sole its branches are:
The Sympathetic Nervous System is a second nervous system, largely independent of the cerebrospinal system and differing from it, in addition to many other points, in the lack of a definite central organ, its nerve cells occurring throughout its peripheral distribution, even in the walls of many organs. For the chief distribution of the sympathetic system is to the viscera. It has a paired arrangement, consisting of a cord-like structure, the sympathetic trunk, situated on either side of the vertebral column or on either side of the median line in front of the column (and therefore ventral to the spinal cord). Each trunk consists of a series of segmental ganglia, the ganglia of the sympathetic trunk, and cord-like interganglionic rami, composed essentially of nerve fibers and connecting the individual ganglia. The number of ganglia is always smaller than that of the vertebrae, especially in the cervical region. The trunk extends through the entire length of the vertebral column; it is wanting in the cranial region, but extends to the anterior surface of the coccyx.
The trunk and its ganglia are connected with the spinal nerves by connections (often double) termed rami communicantes. They permit an exchange of fibers between the cerebrospinal and sympathetic systems and contain the praeganglionic fibers (the only direct connections between the two systems) from the spinal cord. These are less constant and occur less regularly in the cervical than in the thoracic and abdominal portions of the system.
The peripheral plexuses of the system take origin from the sympathetic trunk. Since the system innervates the musculature of the blood-vessels as well as that of the intestine, a part of the peripheral distribution is to these, plexuses, often finely meshed, surrounding the vessels. Only exceptionally do distinct nerves, such as are found in the cerebrospinal system, occur; they have a grey or grayish color.
Cervical, thoracic, abdominal and pelvic portions of the system may be distinguished. The peripheral plexuses in the head region might also be regarded as a cranial portion; they arise, however, from the upper part of the cervical portion of the sympathetic trunk and do not, therefore, constitute an independent portion of the system. Fig. C72, C80, C114, C115, C116, C117, C118.
The cervical portion of the sympathetic trunk possesses as a rule, only three ganglia. It passes downwards behind the common carotid artery, resting on the Longus colli; it itself gives off no branches. The ganglia connect with the cervical nerves by grey rami communicantes.
In addition to the partly sympathetic cardiac plexus (see here), this consists of 11-12 flattened elongated thoracic ganglia lying in front of the heads of the ribs and united by short broad portions of the sympathetic trunk. The upper and lower ganglia are the largest. They are united with the thoracic nerves by rami communicantes, which are frequently double, and send out numerous twigs of variable strength to the descending thoracic aorta, the oesophagus, the pericardium and other structures (vessels, etc.) of the mediastinum; these are termed mediastinal rami. Those passing to the oesophagus make plentiful anastomoses with the thoracic portion of the vagus nerve. Some mediastinal rami also take origin from the splanchnic nerves (see below).
The most important branches of the thoracic portion of the sympathetic trunk are the splanchnic nerves, two long and strong nerves, similar to those of the cerebrospinal system. They consist of a distinctly stronger upper and a weaker lower nerve and they pass to the abdominal cavity. Fig. C18, C22, C115, C116, C117, C118:
These consist of 4-5 lumbar ganglia, 4 (or 5) sacral ganglia and the coccygeal ganglion, and furthermore of the great plexuses of the abdomen and pelvis.
(See here)
The vagus nerve passes through the upper thoracic aperture Into the thoracic cavity, where it lies at first, as in the neck, along the common carotid artery on each side (on the right eventually along the innominate artery). The first. strong branch given off in its course through the thoracic cavity is the recurrent nerve (see here). Since on the left this curves around the aortic arch and on the right around the right subclavian artery, its origin is much deeper on the left than on the right.
The vagus stem on each side now approaches the hilus of the lung, into which it sends numerous strong twigs, which pass along the larger bronchi and so reach the substance of the lung along with bronchial sympathetic rami. Much finer but more numerous twigs from both vagi supply the middle part of the thoracic portion of the oesophagus, again with extensive anastomoses with the mediastinal rami of the sympathetic system. Below the level of the hilus of the lung the vagus ceases as a distinct stem, breaking up into anastomosing cords, the chordae oesophageae, which form a network on the wall of the oesophagus, supplying it and passing with it through the diaphragm. The anterior chorda is formed principally from the left vagus stem and the posterior chorda mainly from the right. In the abdominal cavity the identity of the two stems is preserved only in the innervation of the stomach, and there only approximately; then the vagus fibers so mingle with those of the sympathetic nerves that an anatomical separation of them is impossible.
The central nervous system consists of two portions, very different in form; the brain (encephalon), more or less spherical and contained in the cranial cavity, and the spinal cord (medulla spinalis), cylindrical m form and contained within the vertebral canal.
The spinal cord is almost cylindrical and begins in the region of the decussation of the pyramids, where it is directly continuous with the medulla oblongata. It traverses the vertebral canal to the level of the first lumbar vertebra, giving origin to the roots of the spinal nerves, 8 cervical, 12 thoracic, 5 lumbar, 5 sacral and the coccygeal. In the cervical region it shows a cervical enlargement and in the lumbar region a lumbar enlargement, being much smaller and distinctly cylindrical in the interval between these. The lower end of the lumbar enlargement tapers to a short cone, the conus medullaris, from which a long slender filament, the filum terminate, extends to the end of the sacral canal; it, however, does not contain any nerve tissue. Throughout all the cervical region and in the lumbar enlargement the transverse section of the cord is transversely elliptical. A small, but deep median groove, the anterior median fissure, traverses the entire length of the anterior surface, and, corresponding to this, on the posterior surface is a shallow groove, the posterior median sulcus. On either side are two other grooves, the anterior and posterior lateral sulci, formed by the attachments of the roots of the spinal nerves. In the cervical region there is, in addition, a posterior intermediate sulcus between the posterior median and posterior lateral sulci. Fig. C120, C121, C122, C123, C124, C125, C126, C127, C128, C129.
The portion of the spinal cord on either side between the anterior median fissure and the anterior lateral sulcus is termed the anterior funiculus, that between the anterior and posterior lateral sulci the lateral funiculus, and that between the posterior lateral and median sulci (and the posterior median septum which continues the sulcus into the substance of the cord) is the posterior funiculus. In the cervical region especially the last is divided by the posterior intermediate sulcus (and the septum that continues it) into two portions, the medial fasciculus gracilis (column of Goll) and the lateral fasciculus cuneatus (column of Burdach). The division of the anterior and lateral funiculi into different fasciculi is not evident on the surface of the cord, but the fibres forming the anterior funiculus may be divided into the anterior fasciculus proprius (ground bundle) and a small group of fibres bounding the anterior median fissure, the anterior cerebro-spinal fasciculus (direct pyramidal tract). The lateral funiculus is composed of the lateral cerebro-spinal fasciculus (crossed pyramidal tract), the cerebello-spinal fasciculus (lateral cerebellar tract), the superficial anterolateral fasciculus (Gower's tract) and the lateral fasciculus proprius (ground bundle). (See Fig. C125, C126.)
The grey substance of the spinal cord is in the interior and consists of two symmetrical portions connected by a small bridge of grey matter, in which is the central canal. In front of the canal is an anterior grey commissure and behind it a posterior grey commissure; the former is separated from the floor of the anterior median fissure by a small bundle of crossed fibres, the anterior white commissure. Each half of the grey substance has a large anterior enlargement, the anterior column (horn), and a more slender posterior column (horn), the apex of the latter extending to the surface of the cord. In some parts of the spinal cord there is a lateral projection, the lateral column (horn) which, as the reticular formation, gradually passes into the white substance. Fig. C131, C132, C133, C134S.
The spinal nerves that arise from the cord possess motor anterior roots and sensory posterior roots. The root filaments (fila radicularia) of the anterior roots arise in the anterior column and, separating the anterior and lateral funiculi, come to the surface in the anterior lateral sulcus. The posterior roots arise from the spinal ganglia, situated lateral to the spinal cord, and pass into the cord along the posterior lateral sulcus. Lateral to the ganglia the two roots unite to form a mixed spinal nerve, which promptly divides into a weak posterior and a stronger anterior ramus. The middle and lower spinal nerves leave the cord very obliquely in order to reach their respective intervertebral foramina. Consequently in the lower part of the cord, where the lumbar and sacral nerves arise in immediate succession, there is formed a thick mass of almost parallel nerve stems, the so-called cauda equina, in the center of which is the filum terminale. Fig. C127, C128, C129, C130.
The spinal cord is enclosed within the same membranes as the brain (see here), but the spinal dura mater differs from the cerebral in that it is not fused with the periosteum, but is separated from it by fat tissue and venous plexuses; it also encloses the cauda equina in the sacral canal. The arachnoid lies on the inner surface of the dura mater, separated from it by the slit-like subdural cavity. The pia mater, on the other hand, lies directly upon the surface of the spinal cord, conveys blood vessels to it and sends septa into its substance; in the anterior median fissure it forms a duplicature. It reaches to the end of the cauda equina. In the intervals between successive nerve roots it sends, in the frontal direction, prolongations to the inner surface of the arachnoid, the denticulate ligament; this is wanting between the closely associated nerve roots of the cauda equina. In addition, finer strands and plates of connective tissue unite the pia mater and arachnoid, traversing the subarachnoid cavity and the cerebro-spinal fluid that it contains; in the middle portion of the cord these fibrous bands thicken in the region of the posterior medial sulcus to form the subarachnoid septum. Fig. C120, C121, C122, C124, C130.
According to their course three groups of conducting paths may be recognized in the spinal cord:
Only the first two groups are localized in definite areas of the three funiculi; the fibres of the last group, especially in the anterior and lateral funiculi, lie between those of the other groups.
The cerebral dura mater covers the inner surface of the skull, blending by its outer layer with the periosteum and penetrating for a distance into some of the bony canals for the exit of nerves, such as the internal acoustic pore or the facial canal. The most important structures of the dura mater are:
These lie between the layers of the dura mater, usually in special grooves on the bones. They carry the blood from the cranial cavity and the brain and orbit to the internal jugular vein. Fig. C135, C136, C137, C139, C140, C143. They are:
The cranial pia mater covers the entire surface of the brain, dipping down into the sulci of the cerebral hemispheres. It is the bearer of the principal blood vessels of the surface of the brain. Special developments of it are the chorioid plexuses (see here) and the telae chorioideae of the third and fourth ventricles (see here). Fig. C140, C141, C143, (C190, C191).
The cranial arachnoid, like that of the spinal cord, is a non-vascular membrane, closely applied to the dura mater, separated from it, indeed, by little more than a cleft-like space, the subdural cavity. On the other hand, between the arachnoid and the pia mater, there is a large subarachnoid cavity, filled by the cerebro-spinal fluid, and traversed by numerous connective-tissue strands passing from the pia mater to the arachnoid. Since the arachnoid is associated with the dura rather than the pia mater, it does not follow exactly the surface contours of the brain and does not enter the sulci of the cerebral hemispheres, but enters only those depressions into which the dura mater passes, such as the longitudinal fissure with the falx cerebri, with the tentorium, etc. Fig. C140, C141, C143, C144, C145.
At certain places on the base of the brain, where the brain surface is separated to a greater extent than usual from the inner surface of the dura mater, the subarachnoid space is increased to form cavities, the subarachnoid cisternae, filled with cerebrospinal fluid. The largest of these are as follow:
Furthermore, on the convex upper surface of the brain and especially in the neighborhood of the superior sagittal sinus, the arachnoid forms villous outgrowths which penetrate into the sinus or into its lateral lacunae. Usually these villi form dense tufts, the arachnoidal (Pacchionian) granulations, which cause a thinning of the dura mater and may even break through it so as to lie in corresponding depressions on the inner surfaces of the bones. Fig. C143, C145.
Four large arteries pass to the brain, the two internal carotids from the common carotids (see here) and the two vertebrals from the subclavians (see here); the corresponding arteries of the two sides, as well as the internal carotid and vertebral of the same side, are united at the base of the brain by large anastomoses.
The anterior part of the base of the brain is formed by the frontal lobes of the cerebral hemispheres, separated from one another by the longitudinal cerebral fissure. Its mostly concave surface shows orbital gyri and sulci and, parallel to the longitudinal fissure, the olfactory sulcus, in which lies the olfactory tract with its terminal olfactory bulb, to which branches of the first or olfactory nerve pass from the nasal cavity. The anterior end of the frontal lobe is termed the frontal pole.
Behind the longitudinal fissure is a series of structures which form the floor of the third ventricle, the hypothalamus. These are the optic chiasma, formed by the decussation of the optic tracts; from it arise the optic nerves. On either side of the chiasma is an area with numerous small openings for blood vessels, the anterior perforated substance, at the anterior border of which the olfactory tract arises by several roots. Behind the chiasma is a hollow stalk, the infundibulum, at the end of which is the oval hypophysis. The infundibulum is attached above to a soft grey mass, the tuber cinereum. Behind this, close to the median line, are two small white bodies, the corpora mamillaria, and behind these a depression, the interpeduncular fossa, between the two cerebral peduncles. From this arises on either side, near the middle line, the third nerve, the oculo-motor. The cerebral peduncles are masses of white fibers that issue from the pons; they diverge anteriorly and show distinct longitudinal furrows.
On either side of these structures is the anterior end of a temporal lobe, whose tip is termed the temporal pole; it appears lo be bent around like a hook into the uncus, which extends forwards to the optic chiasma and largely covers in the brain stem, approaching to within 1 cm of the median line.
Behind the corpora mamillaria and the interpeduncular fossa is the broad, white surface of the pons. In the groove between it and the uncus the fourth nerve, the trochlear, comes into view, curving around the brain stem. From the lateral part of the pons the trigeminal nerve arises by a broad sensory portio major and a smaller motor portio minor, which crosses obliquely over the sensory portion. This forms a broad semilunar (Gasserian) ganglion, situated between the two layers of the dura mater at the anterior border of the tentorium, close to the cavernous sinus (see Fig. C60).
At the posterior border of the pons, in the groove between it and the medulla oblongata, the sixth nerve, abducens, arises close to the median line. At the posterior border of the lateral part of the pons, the brachium pontis, passing to the cerebellum, are the origins of the seventh, facial, and eighth, acoustic, nerves and the intermediate nerve lying on the acoustic.
Behind the pons comes the medulla oblongata, which passes over into the spinal cord at the decussation of the pyramids. From the medulla oblongata arise,. between the pyramid and the olive, the root fibres of the hypoglossal nerve (XII) and farther laterally the ninth and tenth nerves, the glosso-pharyngeal and vagus, while the eleventh, the accessory, passes into the skull cavity through the foramen magnum, but receives roots from the medulla oblongata below the vagus.
On either side of the medulla oblongata lie the cerebellar hemispheres and beside and partly behind these the occipital lobes of the cerebral hemispheres, with the occipital poles.
The brain (encephalon) according to its development (see Fig. C150, C151), may be divided into the cerebrum and the rhombencephalon.
The fore brain, telencephalon, forms the greater part of the brain and consists of the pallium, including the hippocampus etc., the corpus striatum, the rhinencephalon, the corpus callosum, the fornix and the septum pellucidum. These together form the cerebral hemispheres; in addition the optic portion of the hypothalamus belongs to it.
The inter-brain, diencephalon, consists of the thalamus, the metathalamus, the epithalamus (these two termed the thalamencephalon) and the mamillary portion of the hypothalamus.
The mid-brain, mesencephalon, consists of the cerebral peduncle and the quadrigeminal lamina.
The hind-brain, metencephalon, includes the pons and the cerebellum.
The after-brain, myelencephalon, is the medulla oblongata.
The two hemispheres are separated by the longitudinal cerebral fissure and the falx cerebri. Their medial surface is flattened. Each hemisphere may be divided into four lobes, frontal, parietal, temporal and occipital. Fig. C152, C153, C154, C155, C156, C157, C158, C159.
The frontal lobes are the anterior portions of each hemisphere, forming its frontal pole. They are separated by the anterior part of the lateral cerebral fissure (fissure of Sylvius) from the temporal lobes; by the praecentral sulcus from the parietal lobes; by the sulcus cinguli from the gyrus cinguli; and by the anterior parolfactory sulcus from the parolfactory area. Fig. C152, C153, C154, C155, C156, C157, C158, C159.
The frontal lobe consists of the orbital gyri, the gyrus rectus, and the superior, middle and inferior frontal gyri. The last of these is divided by the anterior horizontal and anterior ascending branches of the lateral cerebral fissure into opercular, triangular and orbital portions. The sulci are the orbital, olfactory, superior and inferior frontal. Fig. C152, C153, C154, C155, C156, C157, C158, C159.
The parietal lobe forms the middle portion of the cerebral hemisphere and is separated from the temporal lobe by the posterior branch of the lateral cerebral fissure, from the frontal lobe by the praecentral sulcus and from the occipital lobe by the parieto-occipital fissure, this last boundary being lacking on the upper surface of the hemisphere. The principal sulcus is the central sulcus, the principal gyri the anterior and posterior central, bounded by the praecentral and interparietal sulci. These gyri unite on the medial surface of the hemisphere to form the paracentral lobule, which is separated from the praecuneus by the marginal part of the sulcus cinguli. The praecuneus is separated from the occipital lobe by the parieto-occipital fissure and from the gyrus cinguli by the subparietal sulcus. The interparietal sulcus, behind the posterior central gyrus, separates the superior and inferior parietal lobules. At the posterior end of the Sylvian (lateral) fissure is the supramarginal gyrus and at the end of the superior temporal sulcus, the angular gyrus. Fig. C152, C153, C154, C155, C156, C157, C158, C159. At the bottom of the Sylvian (lateral) fissure, covered in by the frontal, parietal and temporal lobes, which form its operculum, is the insula, bounded above arid laterally by the circular sulcus and below by the limen insulae. It has a long gyrus and short gyri. Fig. C160, C161, C162.
The occipital lobe forms the posterior part and the occipital pole of the cerebral hemisphere. Only on the medial surface is it separated from the parietal lobe by the parieto-occipital fissure; elsewhere it passes insensibly into the parietal and temporal lobes. On its medial surface it has the calcarine fissure, which, with the parieto-occipital, bounds the triangular cuneus. Below the calcarine fissure on the concave surface of the lobe is the lingual gyrus, bounded by the collateral fissure, and, below this, the fusiform gyrus, which belongs mainly to the temporal lobe. On the convex surface of the lobe the transverse occipital sulcus separates the superior occipital gyri (and sulci) from the lateral occipital gyri (and sulci), irregularly arranged and highly variable convolutions (microgyri). Fig. C152, C153, C154, C155, C156, C157, C158, C159.
The temporal lobe forms the lower portion of the hemisphere and its temporal pole, which is directed forwards and downwards. On the lateral surface it consists of three parallel gyri, the superior, middle and inferior, separated by the superior and middle temporal sulci. On the concave under surface is the hippocampal gyrus, with the uncus and the fusiform gyrus, the latter being separated from the former by the collateral fissure and from the inferior temporal gyrus by the inferior temporal sulcus. The hippocampal gyrus is continued by the isthmus of the gyrus fornicatus into the gyrus cinguli, situated on the medial surface of the frontal and parietal lobes; the gyrus cinguli and the hippocampal gyrus together form the gyrus fornicatus. (The gyrus cinguli cannot be assigned either to the frontal or the parietal lobe.) Fig. C152, C153, C154, C155, C156, C157, C158, C159.
The corpus callosum is a large, flat mass of nerve fibres, which, as a commissure, unites the two hemispheres and forms the floor of the longitudinal fissure. It consists of a principal part, the trunk, of a posterior thickened portion termed the splenium, which projects over the quadrigeminal plate and forms the upper boundary of the transverse fissure, and of an anterior part, bent upon itself and termed the genu. From the genu, which projects forwards and downwards, there is continued backwards a narrow band, the rostrum, which passes towards the anterior commissure and thence extends as the rostral lamina towards the terminal lamina of the third ventricle. The corpus callosum consists of transverse fibres; on its upper surface there is a thin layer of grey substance which thickens at the median line to form the medial longitudinal striae and laterally, to form the lateral striae. Beneath the anterior part of the corpus callosum (between the trunk and genu) is the septum pellucidum and further back the fornix. Fig. C149, C161, C162, C163, C167, C189, C195, C196, C197, C205.
The fornix is a long, strongly arched, bundle of fibres, whose anterior part forms the columns (pillars) of the fornix, of which a pars tecta and a pars libera may be distinguished. The pars tecta lies concealed in the medial wall of the thalamus and runs from the floor of the third ventricle (from a corpus mamillare) to the anterior surface of the anterior commissure. Here it leaves the substance of the thalamus and runs backwards as the pars libera, rapidly approaching its fellow of the opposite side. It here bounds, together with the anterior part of the thalamus, the interventricular foramen, and it then passes to the under surface of the corpus callosum, from which it is at first separated by the septum pellucidum. Here the two pillars unite to form the body of the fornix and again separate as two flattened bands, the crura, fibres passing traversely from one to the other forming the hippocampal commissure. Each crus accompanies the chorioid plexus downwards and laterally into the inferior cornu of the lateral ventricle, united to the plexus by the taenia fornicis and forming the fimbria of the hippocampus. Thus the fornix fibres connect the hippocampus with the thalamus. Fig. C149, C158, C161, C163, C164, C165, C166, C167, C178, C189, C196, C205.
The septum pellucidum lies between the corpus callosum and the pillars of the fornix, attached to both, and separates the anterior cornua of the two lateral ventricles. It consists of two layers between which is a cleft-like cavity, (the so-called fifth ventricle). Fig. C149, C158, C161, C165, C166, C167, C178, C188, C189, C195, C196, C197, C205.
The rhinencephalon is rudimentary in man. Its peripheral portion (the central rhinencephalon lies within the scope of the pallium) may be divided into anterior and posterior portions. The anterior portion consists of the olfactory tract, lying in the olfactory sulcus of the frontal lobe and enlarging at its anterior end to form the olfactory bulb. The tract begins at the olfactory trigone, situated at the anterior end of the perforated substance, by three white roots, the medial, intermediate and lateral olfactory striae. Fig. C174.
In addition, the parolfactory area, on the medial surface of the hemisphere, below the genu of the corpus callosum, belongs to the anterior portion of the rhinencephalon. It is separated from the superior frontal gyrus by the anterior parolfactory sulcus and from the subcallosal gyrus by the posterior parolfactory sulcus. Fig. C149, C178.
The posterior portion consists of the subcallosal gyrus, Fig. C149, C178, a rudimentary gyrus situated in front of the rostrum of the corpus callosum, of the anterior perforated substance, Fig. C149, and of the limen of the insula, Fig. C174, to which passes the lateral olfactory stria. Fig. C174.
The lateral ventricle lies in the interior of each hemisphere and extends into each of the lobes. The central part in the parietal lobe, below the corpus callosum and at the sides of the corpus striatum, sends off prolongations, the cornua, into the other three lobes. Fig. C163, C164, C165, C166.
The central portion lies immediately beneath the corpus callosum, medial to a club-shaped swelling, the corpus striatum, which, with its caudate nucleus (see below), forms its lateral wall, while its floor is formed by the gray lamina affixa of the thalamus. In the angle between the floor and the corpus striatum is a raised cord, usually of a bluish tinge, the terminal stria, which consists of a tract of fibres and the terminal vein (see here). Anteriorly, where the central portion passes into the anterior horn, it comes into relation with the pars libera of the pillar of the fornix and communicates with the third ventricle by the interventricular foramen (foramen of Monro). On the medial wall is the fornix (see here) and projecting upward from the floor, the chorioid plexus of the lateral ventricle (see here). Fig. C163, C164, C165, C166, C167, C184, C188, C189, C205.
The anterior cornu (horn) extends forward into the frontal lobe, where it ends blindly. It is relatively broad, is covered by the anterior part of the corpus callosum, whose genu forms its anterior boundary. Medially is the septum pellucidum and laterally the portion of the corpus striatum known as the head of the caudate nucleus. The chorioid plexus does not extend into the anterior horn. Fig. C166, C167, C188, C195, C196, C197.
The posterior cornu (horn) is a short, triangular prolongation of the central portion into the occipital lobe, where it lies nearer the medial than the lateral surface, and ends in a point some distance from the occipital pole. Its roof is formed by the occipital radiation of the corpus callosum and, more laterally, by the tapetum, which is also a portion of the callosal radiation. On its medial wall there is a pronounced rounded elevation, the calcar avis, which is produced by the calcarine fissure. Above this there is frequently another elevation, the bulb of the posterior cornu. The posterior cornu is directly continuous with the inferior cornu. Fig. C163, C164, C165, C166, C167, C168, C171.
The inferior cornu (horn) lies in the temporal lobe, nearer its medial than its lateral wall, and is a laterally convex horn-like portion of the lateral ventricle, whose medial wall to some extent is formed only by the ependymal epithelium. This wall is invaginated into the ventricle as the chorioid plexus of the lateral ventricle (see here), the removal of which produces a slit-like opening between the ventricle and the transverse fissure. The inferior cornu communicates with the posterior part of the central portion and with the posterior cornu. The lateral wall and roof are the same as in the posterior horn (callosal radiation and tapetum), the floor is formed by a slight elevation, the collateral trigone, which extends into the posterior cornu between the calcar avis and the hippocampus, and occasionally bears a strong convex, longitudinal ridge, the collateral eminence, produced by the collateral fissure.
The most important structure of the inferior cornu is a whitish, curved swelling, situated on its medial wall, the hippocampus. It begins at the transition of the central portion into the posterior cornu and extends, gradually becoming thicker and broader, too the anterior end of the inferior horn, where it passes into the uncus. Here, where it reaches its greatest thickness, it shows a number of slight prominences, the digitations of the hippocampus (pes hippocampi). The upper medial ends of both hippocampi are connected by the hippocampal commissure, which passes transversely beneath the corpus callosum and the fornix. On the medial surface of the hippocampus and forming its white covering, is the fimbria, the prolongation of the crus of the fornix. On the medial side of the roof of the inferior cornu there is also the tad of the caudate nucleus which, however, does not project into the cavity of the ventricle (see here). Fig. C165, C166, C167, C168, C169, C170, C171, C172, C190. Covered by the fimbria and between it and the hippocampal gyrus is a grey, frequently notched strip, the dentate fascia, which, like the greater part of the fimbria, is really outside the limits of the inferior cornu. The dentate fascia is continuous posteriorly with the fasciola cinerea from the gray covering of the corpus callosum and anteriorly it passes into the so-called band of Giacomini, which unites it to the uncus. Fig. C161, C168, C169, C170, C171, C172, C190.
The choroid plexus of the lateral ventricle has the form of an irregular, contorted band, loosely attached to the floor of each lateral ventricle, and consists of a highly vascular fold of pia mater, covered by the ventricular epithelium. It begins at the interventricular foramen, where it is continuous with the chorioid plexus of the third ventricle, and extends through the central portion of the ventricle and the inferior cornu. At the junction of these two regions it usually has a distinct enlargement, the glomus chorioideum. While the plexus in the central portion of the ventricle is connected with the lateral edges of the tela chorioidea of the third ventricle (see here), in the inferior horn it bulges into the ventricle along a thin strip of the wall beside the hippocampus, carrying with it the greatly contorted chorioid artery (see here), while the corresponding chorioid vein unites with the terminal vein at the interventricular foramen and opens into the internal cerebral vein (see here). The plexus lies laterally to the fornix, to which it is attached, and it is also attached to the lamina affixa of the thalamus (see here) into which its epithelial lining passes, forming the taenia chorioidea. In the inferior cornu the plexus is attached directly to the taenia fimbriae. Fig. C163, C164, C166, C167, C189, C190, C191.
In addition to the grey cortex, each hemisphere contains four masses of grey substance, or ganglia, which, with the exception of the caudate nucleus, are completely imbedded in the substance of the hemisphere. The caudate and lentiform nuclei are connected by their anterior portions and together constitute the corpus striatum.
The third ventricle is an unpaired narrow cavity between the two thalami. Its roof is formed by a layer of epithelium that covers the under surface of the tela chorioidea (velum interpositum). This is a triangular sheet of pia mater; situated beneath the body and the crura of the fornix (see here), and gives rise to the paired but short chorioid plexuses of the third ventricle. Fig. C167, C189, C196. The anterior wall of the ventricle is formed by the pillars of the fornix, the anterior commissure, the rostral lamina of the corpus callosum and the terminal lamina; its floor is formed by the structures of the hypothalamus (optic chiasma, tuber cinereum, corpora mamillaria and posterior perforated substance). Behind, the ventricle gradually passes over into the cavity of the midbrain, its posterior limits being indicated by the epithalamus (pineal body, posterior commissure and anterior end of the quadrigeminal lamina). Its lateral walls are the only boundaries that have any considerable extent and are formed mainly by the thalami, a hypothalamic sulcus indicating the boundary between the thalamus and the. hypothalamus. The ventricle has three outpouchings, two in the region of the hypothalamus, separated by the keel-like projection of the optic chiasma, the third in the epithalamus. In front of the chiasma, between it and the terminal lamina, is the optic recess; behind the chiasma is the somewhat larger infundibular recess, which extends into the stalk of the hypophysis. The epithalamic outpouching, which extends into the pineal body, is termed the pineal recess. Beneath this is the posterior commissure, which connects the two hemispheres. The third ventricle communicates on each side with the lateral ventricle by the interventricular foramen (foramen of Monro) situated between the pillars of the fornix and the anterior ends of the thalamus. Fig. C149, C166, C173, C178, C180, C184, C189, C197, C205.
The thalamus is an elongated, almost oval body, whose rounded anterior end is raised into a small roundish anterior tubercle, while posteriorly it is greatly thickened to form the pulvinar, which overlaps the metathalamus and the lateral surface of the midbrain. The upper convex surface is partly free and covered with pia mater, and partly forms a portion of the floor of the lateral ventricle. It is covered by a layer of white substance, the stratum zonale. To it is attached the lamina affixa, originally a part of the medial wall of the forebrain; it passes as the taenia chorioidea into the epithelial layer of the chorioid plexus of the lateral ventricle (see also here).
The medial wall of the thalamus, slightly convex, lies almost vertically and extends down to the hypothalamic sulcus. It is united with the corresponding surface of the opposite thalamus by a soft, very variable intermediate mass (soft commissure), which passes across the cavity of the ventricle. The boundary between the upper and medial surfaces of the thalamus is a white medullary stria, which is continued posteriorly into the habenular trigone and also into the epithelial roof of the ventricle; when the roof is removed the torn edges of the medullary stria form the taenia thalami. The posterior surface of the thalamus, the pulvinar, is fused with the metathalamus (see here) and the other surfaces are connected with the adjacent parts of the forebrain, the internal capsule, and corpus striatum. Fig. C149, C163, C164, C165, C166, C167, C173, C188, C189, C205.
The hypothalamus forms the floor and the part of the lateral wall of the third ventricle that is below the hypothalamic sulcus. It consists of an anterior optic and a posterior mamillary portion. To the former belong the tuber cinereum, with the infundibulum and hypophysis, the optic tract, with the optic chiasma, and the terminal lamina. The hypophysis consists of an anterior epithelial and a posterior nervous lobe. The terminal lamina is the thin anterior wall of the third ventricle and is continued in front of the anterior commissure into the rostrum of the corpus callosum. The mamillary portion is formed by the two corpora mamillaria each of which contains a grey nucleus. Fig. C148, C149, C157, C161, C174, C177, C178, C179, C205.
The epithalamus consists of the pineal body and its stalk. The pineal body is a grayish-red, flattened, oval body, whose broader base is attached to the posterior part of the roof of the third ventricle, while its apex projects backwards and downwards upon the quadrigeminal lamina. It is connected to the thalamus by the habenulae, which are the direct prolongations of the medullary striae of the thalamus and unite in front of the root the pineal body to form a triangular white plate, the habenular trigone. Into the base of the pineal body there projects the pineal recess, while a slight depression between the pineal body and the tela chorioidea is termed the suprapineal recess. Fig. C149, C165, C173, C178, C180.
The metathalamus is formed by the two geniculate bodies. The more prominent medial geniculate body lies behind the pulvinar, at the anterior end of the inferior quadrigeminal brachium (see below); the less prominent lateral geniculate body is at the posterior lower portion of the thalamus, covered by the pulvinar. The optic tract apparently arises from both bodies, from the medial by a smaller medial root and from the lateral by a stronger lateral root (in reality only the lateral geniculate is an optic center). Fig. C177, C180, C206, C207.
The lower surface of the midbrain is formed by the two cerebral peduncles and by the interpeduncular fossa, in which an anterior and a posterior recess occurs. The roof of the fossa is the posterior perforated substance, which shows numerous openings for blood vessels. The lateral surfaces of the midbrain are formed principally by the cerebral peduncles, the roof by the quadrigeminal lamina. Fig. C148, C149, C157, C173, C174, C177, C178, C206, C207, C212, C213.
The cerebral peduncles are two white bands, which begin at the anterior border of the pons and pass forwards and upwards, above the optic tracts, diverging as they go, to enter the cerebral hemispheres. The under surface of each peduncle is strongly furrowed and is partly visible at the base of the brain, but for the most part it is covered by the optic tract and the hippocampal gyrus and its uncus. Fig. C148, C157, C174, C177, C206, C207, C212, C213.
The quadrigeminal lamina forms the dorsal surface of the midbrain and at the sides passes directly into the tegmentum of the cerebral peduncles. It is a white, rectangular plate, formed by two large anterior superior colliculi and two smaller posterior inferior colliculi, which together form the corpora quadrigemina. From each superior colliculus a white band, the superior brachium, passes to the lateral geniculate body and a similar inferior brachium passes from each inferior colliculus towards the medial geniculate. Behind, the quadrigeminal plate passes over into the brachia conjunctiva of the isthmus, laterally into the upper dorsal portion of the pons. Fig. C149, C165, C173, C178, C180, C188, C206, C207, C212, C213.
The cavity of the midbrain, the aquaeduct (of Sylvius), is a narrow canal about 1½ cm in length, which connects the third and fourth ventricles. In cross section it is triangular or heart-shaped. Fig. C149, C177, C178, C212, C213.
Transverse sections of the midbrain show grey substance in each of the corpora quadrigemina, the nuclei of the superior and inferior colliculi, enclosed by a thin layer of white substance, the stratum zonale. The peduncles in cross section show, below the aquaeduct, the tegmentum, below this on either side an arched or semilunar strongly pigmented area (appearing dark grey in the fresh brain), the substantia nigra, and the basis (crusta). The separation between the two latter portions is shown externally by the lateral sulcus of the midbrain. Fig. C177, C212, C213.
The tegmentum contains in its anterior part a large, round nucleus ruber and, in addition to other small nuclei, numerous longitudinal fibre bundles, which are termed the tegmental bundles. To these belongs the complicated fibre tract known as the lemniscus (fillet), which, divided into a strong medial and a weaker lateral (acoustic) lemniscus, lies lateral to the nucleus ruber. The fibres near the median line cross in the tegmental decussation. An especially large decussation of the brachia conjunctiva occurs beneath the red nucleus. In the grey substance of the floor of the aquaeduct there arises in the region of the anterior colliculi the oculo-motor nerve from the oculo-motor nucleus, and in the region of the inferior colliculi and isthmus, the trochlear nerve. The root fibres of the former traverse the red nucleus and come to the surface at the lateral border of the interpeduncular fossa. Below the nuclei of these two nerves there is a longitudinal fibre tract, ascending from the medulla oblongata, the medial longitudinal fasciculus. Fig. C177, C212, C213.
The basis (crusta) of the peduncles consists of longitudinal fibre bundles, which pass to the internal capsule, principally the pyramidal tracts and the cerebro-pontile tracts. Fig. C212, C213.
The isthmus is formed by the two brachia conjunctiva, the anterior medullary velum and the trigonum lemnisci. The first are flattened white bands, whose fibres connect the cerebellum and the midbrain, passing into the tegmentum. The two brachia converge towards the posterior colliculi and bound a triangular area covered by a thin layer of white substance, the anterior medullary velum. This forms the roof of the upper part of the fourth ventricle and is continuous with the white substance of the vermis of the cerebellum; above it arises a small bundle of fibres, the frenulum, from the groove that separates the two inferior colliculi. Between the brachia conjunctiva, the inferior quadrigeminal brachium and the lateral sulcus of the midbrain there is a triangular area, not always distinctly delimited, which contains the lateral lemniscus (fillet); it is the trigonum lemnisci. Fig. C180, C206.
The cerebrum contains mainly three kinds of conducting paths, which form the greater part of the white substance at the level of the corpus callosum and of the centrum semiovale (Fig. C162) just above. According to their course they fall into three main groups.
The Central Nervous System. The Brain. (Cont.) The Rhombencephalon.
The pons is a broad, convex mass of white fibres situated at the base of the brain. It is separated by a deep transverse fissure from the cerebral peduncles and by a similar fissure, deepened in the median line to form the foramen caecum, from the medulla oblongata. In the median line it is traversed by a shallow groove, the basilar sulcus. The surface of the pons is transversely furrowed on account of the transverse course of its fibres. An oblique fasciculus runs over the lateral slope of the pons towards the brachium pontis, which is a broad mass of fibres which passes to the cerebellum and into which the fibres of the pons gradually pass. Fig. C148, C149, C174, C178, C183, C184, C206, C207.
The medulla oblongata is the direct continuation of the spinal cord and resembles it externally, except that it enlarges above where it takes part in the formation of the inferior part of the rhomboid fossa. Above it is separated from the pons by the transverse fissure mentioned above, while in the rhomboid fossa it shows no line of demarcation. In addition, the medulla oblongata is connected with the cerebellum by the restiform bodies. The anterior median fissure of the spinal cord is continued upon the medulla oblongata to the foramen caecum, interrupted only at the level of the first cervical nerve by the decussation of the pyramids. By the sides of it lie the pyramids, flattened bands formed by the decussation of the lateral pyramidal tracts.
Next these are the lateral funiculi, separated from the pyramids by the continuation upwards of the anterior lateral sulcus of the cord; in the upper part of the medulla oblongata these funiculi enlarge to an elongated anterior elevation, the olive, and to a posterior flat one, the tuberculum cinereum (the prolongation of the posterior column of the cord). On the posterior surface, the posterior median sulcus extends to the obex and the lateral and intermediate posterior sulci are also continued upon the medulla, marking out the fasciculi gracilis and cuneatus. The gracilis ends below the calamus scriptorius in an enlargement, the clava, and the cuneate somewhat higher in a less evident cuneate tubercle. Both funiculi pass into the restiform body, the continuation of the lateral funiculus passing to the cerebellum. Fig. C148, C149, C174, C178, C206, C207.
The fourth ventricle is a flat cavity between the pons and the upper part of the medulla oblongata on the one hand, and the cerebellum on the other. It connects above with the aquaeduct of the midbrain and below with the central canal of the lower part of the medulla (at the calamus scriptorius). Its roof is formed anteriorly by the anterior medullary velum and in part by the brachia conjunctiva, but in its lower portion it is covered in partly by the pia mater, lined with ependymal epithelium and forming the tela chorioidea of the fourth ventricle, and partly by the posterior medullary velum. The former is attached to the margins of the rhomboid fossa by the taeniae of the fourth ventricle; the latter passes into the peduncle of the flocculus of the cerebellum (see here) and meets the anterior medullary velum to form the fastigium. At the calamus scriptorius the taeniae form a projection, the obex. On the ventricular surface of the tela chorioidea there are vascular projections from the pia mater, forming the chorioid plexus of the fourth ventricle, which extends into a lateral outpouching of the ventricle at its broadest portion, the lateral recess, and becomes visible at the base of the brain behind the flocculus of the cerebellum and beside the root of the glossopharyngeal nerve. At this region the ventricle appears to have a paired lateral aperture (inconstant?) and in the median line in front of the obex there is an unpaired medial aperture which is gradually formed during extrauterine life. Fig. C149, C178, C180, C214, C234.
The rhomboid fossa is the floor, or more properly speaking the anterior wall of the fourth ventricle. It is a rhombic depression, pointed above and below, lying on the posterior surface of the pons and medulla oblongata. Its upper point lies in the region of the isthmus, its lower in the region of the myelencephalon, its principal part lying on the dorsal surface of the pons. A superior, an inferior and an intermediate portion may be distinguished, the last being its broadest portion. The lower pointed part of the inferior portion is termed the calamus scriptorius. Throughout the entire length of the fossa there is a posterior median fissure bounded by two elevations, the medial eminences. The intermediate part extends by means of the lateral recess to the ventral surface of the rhombencephalon. It possesses a flat elevation, the acoustic area, which extends partly into the inferior portion and into the lateral recess (here forming the often indistinct acoustic tubercle) and over which variably developed and often plexiform white fibres, the medullary striae, run. Towards the superior portion there is in the region of the medial eminence a rounded elevation, the facial colliculus, corresponding to the genu of the facial nerve. In the upper portion, lateral to the medial eminence, there is an elongated area which has a dark color in the fresh brain and is called the locus caeruleus. The inferior portion has a triangular grey area beside the medial eminence, the hypoglossal trigone, and just below the medullary striae there is another triangular grey area, the ala cinerea (vagus-glossopharyngeus nucleus). Fig. C180, C206, C207, C215, C220, C221, C222.
The cerebellum is a relatively independent portion of the brain, characterized by the conformation of its surface. It differs from the cerebrum by its darker (reddish brown) color and by the close succession and regular arrangement of its surface furrows (see below). It is a transverse, ellipsoidal mass, behind and above the rhomboidal fossa in the region of the medulla oblongata, the pons and the colliculi (partly), and below (and behind) the cerebral hemispheres, being overlapped by their occipital lobes. It is separated from the hemispheres by the tentorium (see here). Its surface is formed of grey substance (cortex) and is divided by very narrow, almost parallel sulci into thin gyri.
The cerebellum consists of a small unpaired middle portion, the vermis, and two paired hemispheres. On their sloping upper surface the hemispheres pass without demarcation into the vermis, which here projects above them (superior vermis), while the inferior vermis is separated from the strongly convex and prominent hemispheres by a deep, broad groove, the vallecula. At the convex borders of the hemispheres the boundaries of the two parts are indicated by flat notches, the anterior and posterior incisures. The cerebellum is united by three peduncles with the neighboring parts of the brain stem, namely, by the brachia conjunctiva (see here) with the midbrain, by the brachia pontis (see here), the strongest of the three, with the pons and by the restiform bodies (see here) with the medulla oblongata. Fig. C148, C149, C178, C183, C230, C231, C232, C233, C234, C235.
Each cerebellar hemisphere is divided by a horizontal sulcus into a superior and an inferior surface. By somewhat deeper sulci the superior surface is divided into the following lobes:
On the more convex inferior surface there may be distinguished:
Each lobule consists of a small, dendritically branched medullary lamina, over whose branchings there is a thin layer of grey cortex (substantia corticalis). The medullary laminae arise from a flattened mass of white substance in the interior of the hemisphere, the medullary body.
Fig. C174, C178, C183, C184, C230, C231, C232, C233, C234, C235.
The Vermis of the Cerebellum is a relatively small, unpaired, medial structure uniting the two hemispheres, and, like these, consists of a central medullary substance, corpus medullare, which projects as medullary laminae into the individual lobes of the vermis, where they are covered by the grey substance of the gyri, forming the arbor vitae.
The superior vermis corresponds to the superior surface of the hemispheres and from before backwards is divided into
The inferior vermis consists of:
Fig. C149, C178, C230, C231, C232, C233.
Just as ganglia are imbedded in the white substance of the cerebral hemispheres, so too in the cerebellum. The largest is the flat dentate nucleus, formed by a thin, folded layer of grey substance enclosed by the medullary substance and also enclosing a portion of it which is connected with the surrounding substance at the hilus. Concentric fibres surround the nucleus, forming its capsule. Near the hilus of the dentate nucleus lies the much smaller, elongated emboliform nucleus and beside this the variable nucleus globosus and, finally, in the roof of the fourth ventricle, the fastigial nucleus. Fig. C234, C235.
In the cerebellum the following are the most important paths:
The eyeball, bulbus oculi, is almost spherical, but its anterior sixth (corneal segment) has a stronger curvature than the rest.
It consists of three concentric membranes, curved in correspondence with the outer surface and enclosing the transparent, partly fluid, partly compact contents of the eye. The outer membrane is the tunica fibrosa, the middle one the tunica vasculosa and the inner one the retina (tunica nervosa). The contents of the eyeball are separated by the iris, formed from the middle membrane, into two principal parts. In front of it lies the anterior chamber (camera) of the eye, whose other boundary is formed by the cornea, the anterior transparent part of the fibrous tunic. Behind the iris there is a firm convex crystalline lens, fastened to the so-called ciliary body of the middle tunic by the zonula ciliaris. Between this and the iris is the small posterior chamber (camera). The entire cavity of the eyeball behind the lens, is filled by the vitreous body (vitreous humor), a semifluid mass.
The outer coat of the eye encloses the entire eyeball as with a capsule and is divided into an anterior, smaller, transparent, strongly curved portion, the cornea, and a larger, posterior, opaque white portion the sclera (sclerotic). The latter is a firm, thick, fibrous membrane, which, in its posterior medial part, is intimately connected with the dural sheath of the optic nerve, while anteriorly it is rather sharply marked off from the cornea, into whose tissue, however, it directly passes over. In the posterior part of the eyeball the sclerotic is distinctly thicker than it is at the equator, and in front of this it is again thickened, owing to the insertion of the rectus muscles of the eyeball.
The sclerotic passes into the cornea in such a way that it forms a sort of groove for the reception of the margin of the cornea (rima cornealis). The groove that indicates the boundary between the sclerotic and cornea on the anterior surface of the eyeball is termed the scleral sulcus. It corresponds closely to a circular venous sinus, the canal of Schlemm, which lies in the sclerotic close to its inner surface. In its posterior part, to the nasal side of the axis of the eyeball, the sclerotic is pierced in a circular area by the bundles of the optic nerve, this area being termed the lamina cribrosa. The inner surface of the sclerotic is united to the middle coat by a thin layer of delicate pigmented tissue, the lamina fusca, an exceedingly thin perichorioidal space intervening. In the region of the so-called pectinate ligament there is an intimate connection of the anterior part of the sclerotic with the margin of the iris.
The cornea is a transparent, saucer-like membrane, which is more strongly curved than the sclerotic. Its surfaces are anterior and posterior; the point of its greatest curvature is the vertex and the border by which it connects with the sclerotic, the limbus.
It is thicker than the sclera and its marginal part is thicker than the central part. Both surfaces are smooth and are almost concentrically curved. The anterior one has a slightly greater area and is covered by the corneal epithelium, which at the limbus of the cornea passes imperceptibly into that of the conjunctiva (see here); the posterior surface is covered by the corneal endothelium and forms the anterior wall of the anterior chamber of the eye.
The middle coat of the eyeball is a thin and soft, pigmented membrane, which carries the blood vessels and the internal musculature of the eye. It consists of three parts. The posterior, which is the chief, is termed the chorioid and is closely applied to the sclerotic. At the point of entrance of the optic nerve it is perforated. The anterior part of the middle coat, the iris, has the form of a diaphragm with a central opening, the pupil, and rests on the anterior surface of the lens. The middle part, which, however, is in front of the equator of the eyeball, is thickened and forms what is called the ciliary body. This is rather firmly attached to the anterior portion of the sclerotic by a ring-shaped thickening, the ciliary anulus.
The chorioid is a thin, pigmented, vascular membrane, whose perfectly smooth inner surface is turned towards the retina, while its rougher outer surface is in contact with the sclerotic. On its outer surface one sees the larger vessels and nerve stems, running for the most part meridionally, and especially the radially arranged venous roots of the vorticose veins. The layer of the chorioid in which the large vessels and nerves lie is termed the vascular lamina, the inner layer the chorio-capillary lamina, since it contains the capillaries. The actual chorioid is not in direct contact with the sclerotic, but is connected with it by a thin pigmented suprachorioidal lamina, both layers of tissue passing into one another; nevertheless the space occupied by the loose lamina is termed the perichorioidal space.
The ciliary body is a ring-shaped thickening of the middle coat, which passes insensibly into the chorioid posteriorly, while the outer border of the iris arises from its anterior part. It consists of a ciliary muscle lying close to the inner surface of the anterior part of the sclerotic and a corona ciliaris. The muscle is a ring-shaped band. triangular in section, in the region of the anulus ciliaris; it consists of external meridional fibres and internal circular ones. The corona ciliaris is the surface turned to the posterior chamber of the eye and the vitreous humor and possesses about 70 radially arranged vascular projections, the ciliary processes, between which is a variable number of smaller ciliary folds. The processes and folds are highest at their anterior ends, in the neighbourhood of the equator of the lens. Their summits are unpigmented and consequently appear as pale lines on relatively dark backgrounds. The orbiculus ciliaris is the posterior part of the ciliary body, which passes insensibly into the chorioid, the boundary between the two corresponding to the ora serrata of the retina.
The iris has the form of a transverse circular disk perforated at the center, whose anterior surface is a boundary of the anterior chamber of the eye, while the posterior is in contact with the lens. The central opening, the pupil, is surrounded by an almost circular, sharp border, the margin of the pupil, while the outer border, the ciliary margin, passes into the ciliary body. It is connected to the inner surface of the sclerotic by the pectinate ligament, this rounding off the angle between the cornea and iris; in the adult it is quite rudimentary.
The anterior and posterior surfaces of the iris have quite different appearances. The anterior surface shows a varying coloration according to the amount of pigment it contains; if it contains little or none, the bluish pigment of its posterior (retinal) layer shows through and it has a bluish color, but if it itself contains pigment, usually in flecks, it has a brownish color. Further, the anterior surface in the region of the pupillary margin possesses fine depressions or crypts, while the much broader ciliary region shows more or less distinctly wavy, radiating striations, wrongly termed folds of the iris, which are due to blood vessels shining through.
The posterior surface is always dark brown or black, since it is covered by the pigmented layer of the inner coat. Further, it has a folded surface, fine, almost concentric, folds being crossed with coarser radiating ones, the latter becoming closer and more numerous towards the pupillary margin. The dark pigment of the posterior surface extends to the border of the pupil and may be seen there as a finely notched border.
The retina consists of two closely applied layers, which pass into one another at the margin of the pupil. The outer pigmented layer is lacking where the optic nerve enters, elsewhere it is present and covers all the parts of the middle layer, such as the ciliary processes etc. The inner layer, the actual retina, consists of two distinct portions; the posterior, thick optic portion, responsive to light, and the anterior caecal portion, which is non-responsive. At the junction of the two portions, about 3-4 mm in front of the equator of the eyeball, there is a notched line, the ora serrata. The optic portion is thickest in the region of the visual axis, where there is a diffuse, yellowish spot, the macula lutea, at the center of which is a sharply defined depression, the central fovea. On the nasal side of the macula there is a slightly elevated white circle, the papilla of the optic nerve.
The caecal portion consists of the ciliary part, covering the inner surface of the ciliary body, and the iridic part, covering the posterior surface of the iris; this portion is pigmented (see here).
The crystalline lens is a biconvex, transparent structure, placed behind the iris and closing the opening of the pupil. Its anterior surface is not so strongly convex as the posterior: the central points of the two surfaces are termed the anterior and posterior poles, and the line joining these the axis of the lens. The margin between the two surfaces is termed the equator and is usually distinctly notched, the notches corresponding to the bundles of the ciliary zonule which are here inserted.
The actual substance of the lens is enclosed within a homogeneous capsule and consists of the nucleus and cortical substance, not clearly separable and formed of lens fibres. The anterior and posterior ends of the lens fibres meet on both the anterior and posterior surface in a star-like figure, which is three-rayed in young individuals, but in later life has several rays, the radii lentis.
The vitreous body fills the large cavity of the eyeball, situated behind the lens; it is spherical in form, but on its anterior surface where it is in contact with the lens it has a hyaloid fossa. It consists of a fluid vitreous humor contained in the meshes of a vitreous stroma, this latter condensing at the surface to form the hyaloid membrane, resting on the inner surface of the retina, but only artificially separable from the rest of the vitreous tissue.
The ciliary zonule is the circular suspensory apparatus of the lens and consists of very delicate, stiff fibres which take their origin from the entire breadth of the ciliary orbiculus and from the intervals between the ciliary processes. The fine fibres collect together to closely set bundles, which pass through the intervals between the ciliary processes to the lens, to whose equator they are attached, giving it its notched form.
The optic nerve passes through the optic foramen above and medial to the ophthalmic artery. It then comes to lie in the axis of the muscle cone, surrounded by the oblique origins of the recti and their tendinous ring, and passes, surrounded by the fat tissue of the orbit, to the medial (nasal) part of the posterior portion of the eyeball. In the orbit it makes a flat S-shaped curve in the horizontal plane, in that it bends first laterally and then returns to the axis of the muscle cone, to make a second very short bend laterally just before entering the eyeball. At about 10-12 mm from the eyeball the central retinal vessels pass into the nerve from below, and run in its axis to the papilla of the optic nerve. As they enter the lamina cribrosa of the sclerotic the nerve fibres lose their medullary sheaths, so that the nerve becomes decidedly thinner and the extremity of the nerve at the optic papilla seems much diminished in size.
The investments of the optic nerve, which are the direct continuations of the brain membranes, are termed its sheath (vagina). Inside the skull cavity the nerve is enclosed in pia only, the so-called pial sheath; at the optic foramen the central dura mater is directly continued upon the nerve forming its dural sheath. Between these two the cerebral arachnoid extends upon the nerve forming its arachnoidal sheath. The cleft-like intervaginal spaces between the sheaths of the nerve correspond to the cavities between the cranial meninges and are in direct connection with them (the subdural and subarachnoid cavities).
The conjunctiva is a mucous membrane, directly continuous with the external skin and lining the conjunctival sac. It consists of the palpebral and bulbar conjunctivae, which pass into one another at the base of the eyelids, forming in the upper lid the superior and in the lower lid the inferior conjunctival fornix. The palpebral conjunctiva covers the inner surface of the eyelid as a smooth membrane, equal in extent to the tarsus (see below) with which it is fused.
The bulbar conjunctiva extends from the conjunctival fornix to the margin of the cornea where it ends in the conjunctival limbus. At the inner angle of the eye it forms a semilunar fold, concave laterally, which forms one of the boundaries of the lacus lacrimalis (see below and Fig. C267).
The two eyelids, the broader upper lid and the narrower lower one, are two folds of skin stretched across the outer opening of the orbit. They have a distinctly concave posterior surface and a convex anterior surface, and bound by their free edges the almost horizontal rima palpebrarum, in such a way as to form at their medial and lateral ends the medial and lateral palpebral commissures. Thus is formed the sharply angled and somewhat higher lateral angle of the eye and the rounded, lower medial angle. The upper lid with a distinctly convex border meets the lower one which has an almost straight and but slightly concave border, in the rima palpebrarum. A strong transverse fold, the orbito-palpebral sulcus, is formed at the base of each lid when it is opened. The free edges that bound the rima palpebrarum are not mere edges, but narrow surfaces, each divisible into the blunt anterior limbus and the sharper posterior limbus, the former bearing 2-3 rows of strong hairs, the eyelashes (cilia).
The lacus lacrimalis is the name given to the region of the medial angle of the eye bounded by the medial portions of the two eyelids and the semilunar fold of the conjunctiva. On its floor there is a low, reddish elevation, with sebaceous glands and fine hair follicles, the lacrimal caruncle.
The support of each eyelid is a cartilage-like plate of connective tissue, the tarsus (see Fig. C284), which is curved in correspondence to the lids. Its form is in general that of the lid, and consequently the higher upper lid has a higher tarsus than the lower. The greatest height of the superior tarsus is at the middle of the breadth of the lid. Both tarsi have an irregular semilunar shape; the medial end is broader than the lateral. One edge of the tarsus is close to the free edge of the eyelid, but the other edge does not extend to the base of the lid but is some distance from it and sharply marked off from the neighboring tissue.
The tarsus of both the upper and the lower eyelid is traversed throughout its entire height by the tarsal (Meibomian) glands, which lie in a single layer, parallel to one another, their ducts opening at slight intervals from one another along the posterior palpebral limbus.
At the angles of the eyelids the tarsi are also connected with the medial palpebral ligament and the lateral palpebral raphe. The former is a tendinous arch attached to the frontal process of the maxilla, and its anterior limb extends transversely over the anterior surface of the lacrimal sac, while the broader posterior limb passes behind the lacrimal sac to the posterior lacrimal crest. It interlaces with the orbital septum (see here) and serves for the fixation of the medial angle. The lateral palpebral raphe is not an actual ligament, but a strip of tendinous tissue that interlaces with the fibres of the Orbicularis oculi and with the orbital septum. The musculature of the eyelids is formed by the palpebral portion of the Orbicularis oculi, whose fibres arch around the rima palpebralis and spread out between the external skin and the anterior surface of the tarsi. The bundles nearest the free edge of the lid, separated from the rest of the muscle by the roots of the eyelashes (cilia), form what is termed the ciliary muscle (Riolan's).
The superior lacrimal gland lies in the lacrimal groove of the frontal bone, close under the periorbita and with its long axis parallel to the margin of the orbit. The surface turned toward the bone is distinctly convex, that turned toward the eyeball concave. The inferior lacrimal gland is only about one-third as large as the superior and lies below it, close to the conjunctival fornix of the lateral angle of the eye. In contrast to the superior one, it consists of only loosely connected, sometimes completely separated, lobules, and its ducts, as well as those of the superior gland, open on the lateral portion of the conjunctival fornix. The number of the ducts of both glands is 10-15.
The lacrimal ducts begin at the puncta lacrimalia on,the edges of the upper and lower eyelids, near the medial commissure of the lids, between this and the medial ends of the tarsi. There is a superior and an inferior punctum, situated on small, low elevations, the lacrimal papillae, on the edges of the eyelids. The lacrimal ducts themselves are very narrow and thin-walled arched canals, situated in the medial portion of the eyelids and running parallel to the boundaries of the lacus lacrimalis. The first part of each runs vertically from its punctum lacrimale, and then follows a bend almost into a transverse direction and at the bend there is an enlargement, the ampulla. The two lacrimal ducts open close together, rarely by means of a common terminal part, into the lateral wall of the lacrimal sac.
The lacrimal sac is the upper, blind end of the naso-lacrimal duct, which is here moderately or not at all enlarged. It lies in the lacrimal fossa at the medial angle of the orbit; its upper, somewhat smaller, blind end is termed the fornix of the lacrimal sac. About 1.5-2 mm below the apex of the fornix the two lacrimal ducts open on a slight evagination of the lateral wall. Above the sac is stretched the medial palpebral ligament, and it, as well as the lacrimal ducts, is also surrounded by the fibres of the lacrimal portion (Horner's muscle) of the Orbicularis oculi. Below, the lacrimal sac is directly continued into the bony canal in which it lies. Like this it opens into the anterior part of the inferior meatus of the nose in such a way, that the duct passes for some distance obliquely through the nasal mucous membrane forming the lacrimal (Basner's) fold.
The movements of the eyeball are produced by six muscles, four of which are termed the recti, and two the obliqui. The four recti have much in common; they are long, flat muscles, becoming broader in front and narrower behind, have a straight course and end in short, fiat tendons, about a centimeter in width, which insert at regular intervals from one another into the sclerotic, in front of the equator of the eyeball and behind the sclero-corneal junction. The two obliqui do not resemble one another so closely, but have this in common, that they run obliquely and their tendons are inserted behind the equator of the eyeball. Five of the six muscles have a common origin at the optic foramen by short tendons from a tendinous ring (Zinnii) which surrounds the optic nerve.
The Rectus superior is the weakest and thinnest of all, and runs with the Levator palpebrae superioris (see here), largely covered by this and partly in close contact with it, above the upper surface of the optic nerve and the upper quadrant of the eyeball to in front of the equator. The lateral part of its tendon remains farther from the margin of the cornea than does the middle part, this reaching almost to the cornea.
The Rectus medialis is the strongest of all the eye muscles, but is shorter than the Rectus superior so far as its fleshy portion is concerned and has a very short tendon, the shortest of all. It is inserted nearest to the margin of the cornea in an almost latitudinal line. It lies in the sagittal plane.
The Rectus lateralis is not placed quite sagittally as is the medial, but inclines temporalwards from this plane. Although it inserts farther away from the margin of the cornea than does the medial, it is necessarily longer than this on account of the convergence of the axes of the orbit posteriorly. The greater length is given, however, solely by the length of the tendon, the fleshy part being, indeed, shorter. The insertion of the tendon is on a latitudinal line, which is much farther away from the corneal margin than is that of the medialis. The muscle arises like the others, chiefly from the tendinous ring, but with a small head (lacertus) from the spine on the border of the superior orbital fissure.
The Rectus inferior lies on the under surface of the eyeball, not exactly opposite the Rectus superior, but inclining nasalwards to the same extent as the latter does temporalwards. The same is true for the moderately long, rather small tendon, which is inserted obliquely as is that of the superior, but in the inverse direction (the lateral border more posteriorly) and somewhat nearer the corneal margin. The length of its fleshy portion is less than that of any of the other recti; nevertheless it is a stronger muscle than the Rectus superior.
For the distances of the rectus tendons from the corneal border, see Fig. C272.
The Obliquus superior arises with the recti from the optic foramen (medial circumference) and from the dural sheath of the optic nerve, and runs forward as a moderately flat muscle in the upper half of the nasal side of the orbit, close under the periorbita and separated from the eyeball by the fatty tissue of the orbit. At first, therefore, it is not in contact with the eyeball, but behind the region of the trochlear spine or fovea of the frontal bone it passes into a round tendon, which passes through a fibro-cartilaginous pulley (trochlea), from which it is separated by a small mucous bursa (trochlear bursa). From the trochlea the tendon, gradually broadening and becoming thinner, runs backwards and laterally, passes under the Rectus superior, and, much broadened, inserts into the eyeball behind its equator. The insertion is a good half centimeter behind that of the Rectus superior and is along an oblique line, mostly on the temporal side and running almost parallel with the axis of the optic nerve.
The Obliquus inferior is the only one of the six muscles that takes its origin from the anterior portion of the orbit. It arises by a small and short tendon from the posterior part of the infraorbital border of the maxilla, below the fossa for the lacrimal sac. It runs, becoming somewhat broader, obliquely beneath the lower part of the eyeball, crosses under the Rectus inferior (lying between it and the Rectus lateralis) and passes, like the Obliquus superior, to the temporal side of the posterior hemisphere of the eyeball. Here it inserts opposite the tendon of the Obliquus superior, but by a smaller and shorter insertion, in a line which crosses the axis of the eyeball at an acute angle. It is by far the shortest of all the eye muscles; its tendon is usually very short.
The eye muscles are provided with a fascial investment in the anterior part of their length, but in the cases of the Recti and the Obliquus superior this sheath becomes gradually thinner posteriorly, so that the posterior portion of these muscles lies practically naked in the fat tissue of the orbit. The stronger anterior part of the sheaths of the Recti is only apparently a direct continuation of Tenon's capsule (see here). Only the Obliquus inferior has a uniformly thick fascia throughout its entire length, as has also the praetrochlear portion of the tendon of the Obliquus superior, whose sheath is a direct tubular prolongation of Tenon's capsule.
In addition to the six muscles that move the eyeball there is in the orbit another transversely striated, voluntary muscle, the Levator palpebrae superioris. It is a long muscle, broader in front than behind, which almost covers the Rectus superior (only its lateral border remains free) and lies closely imposed upon that muscle in the posterior part of the orbit. It arises with the Rectus superior by a small, short tendon from the tendinous ring (see here), it consists of striated muscle tissue and is covered by fascia in its anterior portion. Between its tendon and the palpebral conjunctiva there are the smooth muscle fibres of Muller's muscle, m. palpebralis. The aponeurosis forks before its insertion in such a way that the posterior part inserts into the upper border and the whole anterior surface of the tarsus of the upper lid, while the anterior part passes between the tarsus and the skin of the eyelid and inserts into this skin.
The term m. orbitalis is applied to smooth muscle fibres of the orbit which occur in variable amount around the eyeball and also form a strong layer closing the inferior orbital fissure.
The periorbita is the periosteal lining of the orbit and is continuous with the periosteal layer of the dura mater at the optic foramen and superior orbital fissure, and with the periosteum of the bones of the face at the inferior orbital fissure. The superior orbital fissure is closed by a thickening of the periorbita, except for the openings for the passage of blood vessels and nerves.
The orbital septum is a fascia-like, connective tissue structure at the opening of the orbit, like a diaphragm perforated at its center. It covers the posterior surfaces of the eyelids, follows their form and is therefore convex anteriorly, and separates them from the actual contents of the orbit. At the same time it is the posterior fascia of the Orbicularis oculi. Since it extends into the bases of the eyelids it belongs to a certain extent also to these and, in the upper lid, it is connected with the aponeurosis of the Levator palpebrae superioris. The nerves and blood vessels passing out from the opening of the orbit (the frontal, supraorbital, supratrochlear, infratrochlear and lacrimal nerves; the frontal and supraorbital arteries and the naso-frontal vein) pierce the upper (orbital) part of the septum. At the medial and lateral angles of the eye it is connected with the medial palpebral ligament and the lateral palpebral raphe. It shuts in the fat tissue (corpus adiposum) of the orbit anteriorly and is made convex anteriorly by it.
Tenon's capsule is a hollow spherical structure, formed of lamellae of connective tissue, in which the posterior hemisphere of the eyeball rests and moves. It separates the eyeball from the fat tissue of the orbit. The anterior thickened end of the capsule lies at the fornix of the conjunctiva and splits there into a conjunctival and a palpebral portion. Posteriorly the capsule gradually becomes thinner. It is pierced in the first place by the optic nerve, and, secondly, by the tendons of the six muscles of the eyeball. The optic nerve passes through an irregularly round opening in the posterior thinner portion of the capsule and with it pass the accompanying nerves and vessels (ciliary nerves and vessels), so that the capsule becomes gradually inseparably united with the sclerotic. The muscle tendons pierce the capsule (here markedly thicker) obliquely through slit-like openings and, from the openings for the obliqui, the capsule extends backwards over the tendons of these muscles as a strong fascia (see here).
The capsule is not in immediate contact with the eyeball, but throughout its entire extent is separated from it by a narrow space (interfascial space), traversed by strands of connective tissue. Anteriorly this space extends to behind the bulbar conjunctiva.
The auditory apparatus, which is mostly contained within the temporal bone of the skull, may be divided into three principal portions:
The membranous labyrinth is a branched, exceedingly thin-walled system of canals, filled by a watery fluid, the endolymph. The following parts may be distinguished in the endolymphatic canal system: the two vestibular sacs, the sacculus and utriculus, which are only indirectly connected with one another by the utriculosaccular duct, this arising from the endolymphatic duct, which, again, is a slender, blindly ending process from the sacculus. From the larger of the two sacs, the utriculus, three arched semicircular canals (ducts) take origin, while a spiral canal, the cochlear duct, is connected with the sacculus by a short, narrow canal, the ductus reuniens.
The endolymphatic ducts lie in corresponding cavities of the bony labyrinth, without, however, completely filling them. Between the membranous and bony labyrinths there is a perilymphatic space, also filled with fluid, the perilymph.
The utriculus is an oval, slightly flattened sac, which lies in the hemielliptic recess of the bony labyrinth. The semicircular canals (ducts), which arise from it, are very thin-walled endolymphatic canals, oval in section, which lie eccentrically in similar bony canals. One canal is superior (anterior), another lateral (horizontal) and the third posterior, and each has a hemispherical enlargement, an ampulla, at one of the ends attached to the utriculus, the ampulla of the superior canal being at its anterior end, that of the posterior canal at its lower end and that of the lateral canal at its anterior end. The membranous ampullae fill the bony ampullae almost completely. Corresponding to the relations of the bony canals, only the lateral canal has two separate openings into the utriculus, the superior and posterior canals, in addition to their openings through the ampullae, open at their other end by a very narrow common limb.
The sacculus is the smaller of the two vestibular sacs, and lies in the hemispherical recess of the bony vestibule. It has the form of a flattened sphere. From its lower slightly smaller end arises the very narrow ductus reuniens by which it communicates with the cochlea.
The cochlear duct is a narrow, spirally coiled canal, triangular in section, and runs in the spiral canal of the cochlea, making two and a half turns about the cochlear axis. It begins while still in the region of the vestibule by a blind sac, the vestibular caecum, and ends at the apex of the cochlea in the cupular caecum. One of its walls is attached to the free edge of the bony spiral lamina and extends to the opposite wall of the cochlea, where it unites with a periosteal thickening, the so-called spiral ligament; this wall is the membranous spiral lamina and it separates completely the scalae of the cochlea (see here), which, without it would pass into one another at the free edge of the bony spiral lamina. A second wall is continuous with that just described over a thickening of connective tissue, the limbus spiralis, near the free edge of the bony spiral lamina, and extends thence as the very thin vestibular (Reissner's) membrane to the opposite wall of the cochlea, separating the cochlear duct from the perilymphatic scala vestibuli. The third wall is adherent to the lateral wall of the bony cochlea, completing the triangular cochlear duct (see Fig. C288).
The endolymphatic duct and sac are very rudimentary in man. The former arises from the lateral part of the sacculus and extends as an exceedingly fine canal through the whole length of the aquaeductus vestibuli, emerging under the dura mater to end blindly in the endolymphatic sac. Soon after leaving the sacculus the duct is joined at an acute angle by the utriculosaccular duct.
The internal auditory (acoustic) meatus begins at the internal auditory (acoustic) pore on the pyramid of the temporal bone and passes laterally in the substance of the bone, to end in the fundus. At this floor of the meatus the two nerve trunks, the facial and acoustic, which it contains, separate. On the fundus there is an almost horizontal transverse crest, which separates an upper smaller area from a lower larger one. The anterior part of the upper area is the area of the facial nerve and on it the facial canal begins at a rather large, round foramen. The posterior part of the upper area, the superior vestibular area, shows a number of small foramina which lead to the superior macula cribrosa of the vestibule (see here) and contain the utricular and superior and lateral ampullary branches of the acoustic nerve. Below the transverse crest anteriorly is the cochlear area, which has a number of foramina arranged spirally, lying in the hollow base of the axis of the cochlea. Posteriorly is the inferior vestibular area, also with small foramina which lead to the middle macula cribrosa of the vestibule the saccular branch of the acoustic nerve. Finally there is an isolated round foramen singulare towards the posterior wall, that leads to the inferior macula cribrosa and transmits the posterior ampullary branch of the acoustic nerve.
The cochlea has the form of a spiral canal with two and a half turns. Its coils pass for the most part around an axis, the modiolus, which is formed of spongy bone and has the form of a low hollow cone. The broader part of the cochlea is its base and the apex, the cupula. The latter is directed towards the tympanic cavity, close to the medial wall of the tuba auditiva; the base looks towards the internal auditory pore. Consequently the axis of the cochlea lies obliquely, almost perpendicular to the posterior surface of the pyramid (see Fig. C293). The bony cochlear canal begins in the vestibule and near its beginning communicates with the tympanic cavity through the cochlear fenestra, and makes an elevation, the promontory, upon the lateral wall of that cavity. It runs free for a short distance (marked by * on Fig. C296) before it begins to coil about the modiolus. Towards the cupula it becomes gradually narrower; the middle coil is seated on the basal one and lies at a higher level; the apical coil, on the other hand, is surrounded by the middle coil.
The base of the modiolus is formed by the cochlear area at the fundus of the internal auditory meatus and contains the spiral tract of foramina for the entrance of nerve fibres. The axis of the modiolus coincides with that of the cochlea, but is much shorter. The basal coil of the spiral canal bends around the hollow base of the modiolus; in the region of the middle coil the modiolus consists of spongy bone, traversed by narrow longitudinal canals that end blindly; at the end of the second coil the modiolus proper ends and is continued by the lamina modioli. Around the modiolus winds the bony spiral lamina, which is an incomplete partition of the spiral canal. Where the modiolus ends the bony spiral lamina becomes free and curves as a thin sickle-shaped plate, the hamulus, around the lamina modioli. There is thus formed between the lamina modioli and the hamulus a semilunar helicotrema, through which the two scalae, separated by the cochlear duct, communicate. The lower scala tympani begins at the cochlear fenestra and lies below the spiral lamina, while the upper scala vestibuli begins at the cochlear recess of the vestibule and runs above the vestibular membrane. At the beginning of the basal coil there appears on the lateral wall opposite the spiral lamina a secondary spiral lamina, which does not, however, extend beyond the basal coil. Since the half of the apical coil does not project above the level of the middle coil, the position of the bony wall between the coils changes. Between the basal and middle coils the thick intervening wall formed by the base of the modiolus is perpendicular to the axis of the modiolus; already in the middle coil it becomes oblique to it, and in the apical coil it comes to lie in the plane of the axis of the cochlea forming a plate, the lamina modioli, which is concave towards the apical coil, convex towards the middle coil. (Fig. C300.)
The bony semicircular canals contain the membranous ones and, as in the case of these, two are vertical and one horizontal. Each describes about two-thirds of the circumference of a circle and their lumina are flattened in their planes of curvature. Each canal communicates with the vestibule by two openings, a wider ampullated and a narrower simple one, but the two vertical canals are united for a certain distance to form a common, non-ampullary limb, so that there are really only five openings into the vestibule. The superior (anterior vertical) canal is perpendicular to the axis of the pyramid of the temporal bone and, accordingly, parallel to its transverse diameter. It is also higher than the others, the highest point of its curve lying immediately beneath the arcuate eminence of the anterior surface of the pyramid. It begins at its anterior end with an ampullary limb, dilated to form the superior ampulla and at its posterior end forms with the posterior canal the common limb. It is narrower and longer than the lateral canal but somewhat broader and shorter than the posterior.
The second vertical canal, the posterior, is almost parallel to the posterior surface of the pyramid of the temporal bone and is at right angles to the superior canal. Its strongest curvature looks backwards and downwards. It begins at the vestibule by an ampullary limb, its ampulla opening on the lower wall of the vestibule at some distance from the other two ampullae. Its upper end unites with the posterior end of the superior canal to form the common limb. The posterior canal lies more deeply than the superior; it is the most strongly curved of all the semicircular canals and is consequently the longest, but also the narrowest.
The horizontal lateral canal lies horizontally in the angle formed by the two vertical canals. It is by far the shortest of the three, but also the broadest. Furthermore, it has two separate openings into the vestibule; the ampullary limb is the anterior one and begins in the lateral ampulla, close beside the superior ampulla and forming the prominence of the lateral canal; the posterior limb opens into the vestibule below the common limb. The apex of the curvature of the canal looks laterally and somewhat backwards.
The vestibule is the middle portion of the bony labyrinth, situated between the semicircular canals and the cochlea. Its medial wall borders upon the internal auditory meatus and its lateral wall on the tympanic cavity, an opening on this wall, the fenestra vestibuli (ovalis), placing this cavity in communication with the vestibule (see also here).
On the anterior wall is an almost vertical, low ridge, the vestibular crest, which separates a small, round, anterior (and inferior) depression, the hemispherical recess, from a larger elongated, posterior (and superior) one, the hemielliptic recess. The former lodges the sacculus, the latter the utriculus. The vestibular crest terminates above in a sharp projection, the pyramid, and below in two limbs that bound a flat depression. This depression, the cochlear recess, is really in the lower wall of the vestibule, close to the beginning of the spiral lamina (see here); it lodges the vestibular caecum of the cochlear duct (see here).
In addition to the kidney-shaped fenestra vestibuli (ovalis) and the round fenestra cochleae (rotunda), there are other openings in the wall of the vestibule for the passage of branches of the acoustic nerve. In the lateral wall, in the region of the hemispherical recess, there is a number of small foramina, forming the middle macula cribrosa, through which pass nerve twigs for the macula acustica of the sacculus. A similar area, the superior macula cribrosa, lies at the upper end of the vestibular crest for the utriculo-ampullary nerve, while the smallest, the inferior macula cribrosa, which corresponds to the foramen singulare, is situated beside the ampulla of the posterior semicircular canal, on the lower surface of the vestibule. The five openings of the semicircular; canals open into the posterior portion of the vestibule, three being ampullary openings and two non-ampullary (see here). The latter lie in the medial wall of the vestibule, that of the lateral canal below that of the common limb. The ampulla of the posterior canal is on the lower wall; the other two ampullae are close together at the boundary between the posterior and lateral walls.
Furthermore the spiral canal of the cochlea opens on the anterior wall and the vestibular aquaeduct on the medial wall by an elongated fine slit.
The medial (labyrinthic) wall of the tympanic cavity presents its most important structures. At about its middle is the fenestra vestibuli (ovalis), which is kidney-shaped, convex above and concave below, and lies in a niche-like depression, the fossula of the fenestra vestibuli. Immediately beneath the fenestra is a rounded eminence, the promontory, formed by the basal coil of the cochlea, and over its surface a groove runs from above downwards. Below and behind the promontory and almost concealed by it is a second, roundish opening, the fenestra cochleae (rotunda), in a rather deep depression, the fossula of the fenestra cochleae, its sharp border being termed the crest of the fenestra rotunda. The fossula is bounded posteriorly by a ridge-like swelling that has its origin at the fenestra vestibuli (ovalis), the subiculum of the promontory. Above it is a small depression, the tympanic sinus, and near the anterior end of the fenestra vestibuli (ovalis) there is a curved, spoon-like projection, the cochleariform process, which is the free end of the septum of the musculo-tubar canal.
The posterior (mastoid) wall of the cavity is mostly occupied by the openings of the mastoid cells, the largest of these cavities, opening directly into the tympanic cavity, being termed the mastoid antrum. In addition there is on the posterior wall, above the fenestra vestibuli (ovalis) a distinct, elongated projection, the prominence of the facial canal. Above this is a stronger eminence, the prominence of the lateral semicircular canal, corresponding to the ampulla of that canal. Behind the fenestra vestibuli (ovalis) and in front of the lower portion of the prominence of the facial canal is a small, conical, hollow elevation, the pyramidal eminence. Above this is a small but deep depression, the posterior sinus, and above this again a shallow depression, the fossa incudis, for the short limb of the incus. In addition, on this wall is the opening for the passage of the chorda tympani into the tympanic cavity.
The anterior (carotid) wall possesses the opening of the musculo-tubar canal and also the small openings of the carotico-tympanic canaliculi from the carotid canal. The lateral (membranaceous) wall is essentially a round opening closed by the tympanic membrane and above this by a small plate of bone, behind which is the head of the malleus and a part of the body of the incus. The upper (tegmental) wall has a shallow depression, the epitympanic recess, which deepens dome-like towards the lateral wall to form the pars cupularis. The lower (jugular) wall frequently shows opposite the point of attachment of the styloid process a low tubercle, the styloid prominence. On all the walls of the tympanic cavity, except on the promontory and the epitympanic recess, there are groove-like depressions, the tympanic cellules, which extend as the tubar cellules into the beginning of the tuba auditiva.
The malleus has the form of a mallet. It has a rounded head (capitulum), a constriction below this, the neck (collum), and a handle (manubrium), as well as two processes. The head is rounded at its upper end and on its posterior surface has an articular facet for the incus. The neck is below this facet. The manubrium lies approximately in the line of prolongation of the head and is a long cylindrical rod of bone which is attached throughout its entire length to the tympanic membrane, its end corresponding to the umbo of the membrane. It is not actually a direct prolongation of the head and neck, but forms with this an angle of 125-150°. Of the two processes of the malleus the lateral process lies at the base of the manubrium, where it forms a short thick process, which produces the malleolar prominence of the tympanic membrane. The anterior (Folian) process is a long, thin, spicule of bone, usually much longer in the new-born child than in the adult, where it is occasionally quite rudimentary. It arises from the anterior surface of the neck and extends towards the petro-tympanic fissure, imbedded in the anterior ligament of the malleus (see here).
The incus has almost the shape of a molar tooth, with two roots of unequal length. It has a body (corpus) and two limbs (crura) that taper towards their ends. The body looks forward and has on its surface a saddle-shaped depression for the reception of the malleus. The long crus lies almost parallel and medial to the manubrium of the malleus, but behind it. It is shorter than the manubrium and bears at its end a disk-shaped enlargement, the lenticular process. The short crus looks towards the tympanic antrum and is almost horizontal. Its blunt end rests in the fossa incudis of the tympanic cavity.
The stapes corresponds in shape very perfectly to its name (stirrup). It consists of a flat, oval foot-plate (basis), which fits into the fenestra vestibuli (ovalis), and two limbs (crura), which pass almost horizontally from the two ends of the foot-plate, a somewhat shorter, less curved anterior crus and the more strongly curved, posterior crus. These meet at the head (capitulum) of the stapes. The bone has a small articulating surface for the lenticular process of the incus.
The three auditory ossicles are united by two articulations. The articulation of the malleus with the incus is a saddle-shaped joint. The head of the malleus has a markedly convex articular surface, covered by cartilage, and the surface of the body of the incus is correspondingly concave; a delicate articular capsule encloses the two surfaces. Each of the two surfaces possesses, in addition, a spur-like process below it. The joint between the incus and stapes is between the lenticular process of the incus and the capitulum of the stapes. It is an ellipsoid joint, approximating a ball and socket. The stapes lies with the plane uniting its two crura almost at right angles to the long axis of the long crus of the incus.
In addition to these articulations there is the so-called tympano-stapedial syndesmosis, the union of the base of the stapes with the fenestra vestibuli (ovalis). The fenestra is closed by the periosteum of the tympanic cavity and the small space between its bony margin and the base of the stapes is filled by ligament.
For the fixation of the malleus there are three ligaments. The superior (Fig. C315, C317, C318) fastens the head of the malleus in the epitympanic recess to the under surface of the tegmen tympani. The lateral (Fig. C314) passes from the margin of the tympanic membrane to the malleus, where it inserts at the base of the two processes of the bone. The anterior surrounds the anterior (Folian) process of the malleus and seems to be a continuation of this; it passes to the petro-tympanic fissure and through this to the angular spine of the sphenoid bone. In addition, the manubrium is attached to the tympanic membrane.
The incus is held in position by the following ligaments. The superior (Fig. C317, C318) extends from the body of the incus to the roof of the tympanic cavity; the posterior (Fig. C314, C315, C316, C317, C318) is a short dense ligament fastening the short crus of the incus in the fossa incudis of the tympanic cavity.
A thin membrane stretched between the two limbs of the stapes is termed the obturator membrane (Fig. C319).
The Tensor tympani is an elongated muscle which lies in a canal forming the upper part of the musculo-tubar canal. It arises from the walls of its canal, and also from the cartilage of the tuba auditiva (Eustachian tube) and the neighborhood of the sphenopetrous fissure. As it runs through its canal it is enclosed by a strong layer of periosteum (Fig. C323) until it almost reaches the tympanic cavity. At the root of the cochleariform process it becomes converted into a round tendon, which, running through the spoon-like concavity of the process, bends almost at a right angle and passes almost transversely through the tympanic cavity to be inserted on the medial side of the base of the manubrium of the malleus, opposite the lateral process. The muscle draws the tympanic membrane inwards towards the tympanic cavity and by doing so tenses it (Fig. C318, C319, C320, C321, C323, C324).
The Stapedius (Fig. C320) is smaller than the Tensor tympani; indeed it is the smallest skeletal muscle in the body, hardly over 1 mm in length. It has an elongated conical form and lies completely enclosed within the cavity of the pyramidal eminence, from whose walls it arises. It passes into a short, thin tendon, which passes through the small opening at the apex of the pyramid and is attached to the posterior crus of the stapes close to the capitulum. As it passes out of the cavity of the pyramid the tendon is bent downward somewhat. Its function is uncertain.
The tympanic cavity (Fig. C314, C315, C316, C317, C318, C319, C320, C321, C322, C324) is lined throughout its entire extent by a very thin and delicate mucous membrane, which extends also into the mastoid antrum and into the mastoid cells, and becomes continuous with the pharyngeal mucous membrane through the tuba auditiva (Eustachian tube). In general it lies close upon the bony walls of the tympanic cavity and upon the auditory ossicles, and follows the outlines of these parts. But it also forms some folds projecting into the cavity. Many of these are variable, but in the vicinity of the tympanic membrane and malleus there are two strong, constant, semilunar folds. There is an anterior malleolar fold (Fig. C316, ), that contains the chorda tympani, the anterior ligament and process of the malleus; it arises from the greater tympanic spine (see here) and is attached to the neck of the malleus. The posterior malleolar fold (Fig. C316, C317, C318) contains the chorda tympani after it has entered the tympanic cavity, and extends from the lesser tympanic spine to the neck of the malleus. It lies close to the tympanic membrane and is continuous in part with its mucous layer.
The plica incudis passes from the long crus of the incus to the posterior wall of the tympanic cavity; the stapedial fold covers the tendon of the Stapedius, the stapes and its obturator membrane. Small folds cover the secondary tympanic membrane that closes the fenestra cochleae (rotunda). The tendon of the Tensor tympani also runs in a fold.
Partly as a consequence of these folds and partly on account of the conformation of the bones forming the walls of the tympanic cavity, there is formed a series of blind pouches. The cleft-like pouches opening downwards that the malleolar folds make with the tympanic membrane are termed the anterior and posterior recesses of the membrane. A superior recess (Prussak's space) is a narrow space lying between the pars flaccida of the membrane and the neck of the malleus. It is closed below by the lateral process of the malleus and its upper boundary is the lateral ligament of the same bone; it communicates with the posterior recess. The space in which the head of the malleus and body of the incus are situated above the tympanic membrane is termed the epitympanic recess (Fig. C326). It is bounded by a bony plate of the lateral wall of the tympanic cavity and by the cupula of the tegmen tympani, and is at least partly separated from the recesses of the tympanic membrane by the lateral ligament of the malleus.
(Fig. C314, C315, C316, C317, C318, C319, C320, C321, C323, C330, C331.)
The tuba auditiva (Eustachian tube) is about 3½ cm in length and places the tympanic cavity in communication with the naso-pharyngeal cavity. It has two portions, the one, the bony portion, lying in the substance of the petrous portion of the temporal, the other, the cartilaginous portion, lying in the roof and wall of the pharynx.
The inner surface, throughout both portions, is lined by mucous membrane. The narrowest part of the tube lies at the transition from the bony to the cartilaginous portions and is termed the isthmus of the tube.
The bony portion of the tube begins in the anterior wall of the tympanic cavity and follows the course and form of the bony canal, which is separated by the septum of the musculotubar canal from the Tensor tympani (see here). Its transition into the cartilaginous portion takes place in the region of the spheno-petrosal fissure.
While the cartilaginous portion has a narrow cleft-like lumen, that of the bony portion, corresponding with the caliber of the bony canal m which it lies, is relatively wide and rounded triangular. The bony portion lacks glandular structures in its very thin mucous membrane; on the other hand, like the bony canal for the Tensor tympani (see here), it possesses numerous small blind pockets, the tubar cells.
The cartilaginous portion extends from the isthmus to the opening into the pharynx. Its cartilage is low and small at the transition into the bony part and surrounds the lumen completely. Towards the opening into the pharynx the cartilage becomes thicker and higher, but it serves as a support for the tube in this part of its course only on its upper and medial wall, having now assumed the form of a curved plate that forms a narrow groove. The plate consists of a lateral and medial lamina (Fig. C329, C330, C331), but these are continuous above over the groove which opens downwards. The medial lamina, towards the opening into the pharynx becomes higher and noticeably thicker than the lateral one, which extends as a hook-like bent plate only into the upper part of the lateral wall of the tube, the lower part of this wall and the lower wall being formed by the membranous lamina (Fig. C331). The lumen of the cartilaginous part of the tube is merely a vertical cleft (Fig. C330, C331). The medial lamina is especially thickened at the opening into the pharynx and forms there the projecting torus tubarius.
The tympanic membrane (Fig. C318) is a very thin, but dense and tense membrane, almost circular or elliptical, which closes the tympanic cavity laterally and consequently forms the boundary between the middle and external ear. In the adult there is a groove, the tympanic sulcus, in the tympanic portion of the temporal bone where the membrane is attached, but the upper quarter of its attachment is to the squamous portion of the temporal, in the tympanic notch, which is bounded on either side by the tympanic spines (greater and lesser) (Fig. C326). In the tympanic sulcus the membrane is fastened by a circular thickening, the fibrocartilaginous ring, which is really the margin of the membrane.
The surface of the tympanic membrane that is turned towards the lumen of the external auditory meatus is covered by the external skin, greatly diminished in thickness, while the surface turned towards the tympanic cavity is covered by mucous membrane.
The tympanic membrane shows two distinctly different portions, a greater tense portion and a smaller flaccid portion, the latter corresponding to the attachment in the tympanic notch. The tense portion is drawn inwards funnel-like towards the tympanic cavity by the attachment of the manubrium of the malleus to it, and the depression which thus results on the outer surface of the membrane is termed the umbo (Fig. C327). This surface when seen through the external meatus is shining and the entire length of the manubrium of the malleus shows through as a white streak, the malleolar stria. Since the top of the manubrium reaches to below the center of the tympanic membrane, the umbo is slightly eccentric. At the upper end of the malleolar stria is a slight projection, the malleolar prominence, produced by the lateral process of the malleus, and above this the flaccid portion of the membrane begins (Fig. C327). The manubrium of the malleus is so fastened to the medial surface of the membrane, that the mucous membrane of the tympanic cavity passes over both, and from the malleolar prominence curved folds which separate the tense and flaccid portions of the membrane extend, the anterior, shorter one (plica anterior) to the lesser tympanic spine and the posterior longer one (plica posterior) to the greater spine (Fig. C327).
The tympanic membrane is placed obliquely with reference to the axis of the external auditory meatus, indeed, it is oblique in two directions. In the first place the anterior border of the membrane is more medial than the posterior, whereby the anterior wall of the meatus is distinctly longer than the posterior wall. Furthermore, the upper border of the membrane lies further forward than the lower border. Consequently, the membrane is oblique both in the vertical and in the horizontal plane and, in addition, it has the funnel-like form produced by the umbo. The upper and lower segments of the funnel form different angles with the wall of the meatus, the upper one an obtuse angle and the lower an acute.
The external auditory (acoustic) meatus consists of two portions, a medial bony portion and a lateral cartilaginous portion, which pass the one into the other, without interruption. The bony portion extends from the external auditory (acoustic) pore to the groove for the tympanic membrane in the tympanic portion of the temporal bone and, since the tympanic membrane is placed obliquely to the axis of the meatus, the upper wall of the meatus is shorter than the lower one and the posterior wall shorter than the anterior. The cartilaginous portion of the meatus is a part of the cartilaginous framework of the auricle.
The meatus lies almost in the frontal plane and horizontally, and runs almost directly medially between the auricle and the tympanic membrane; its departure from the horizontal direction is but small, that from the frontal direction somewhat greater. Furthermore the course of the meatus is by no means straight, but shows individual and variable bendings, that are mainly in the cartilaginous portion. One bend lies close behind the entrance and looks upwards and forwards and a second bend is near the boundary between the bony and cartilaginous portions and looks backwards and downwards, but is less marked than the first bend. The bony part then carries the direction somewhat forward again.
In its length the meatus shows individual differences; on the average it is 35 mm, the bony part forming 1/3 and the cartilaginous part 2/3. In transverse section it is in general irregularly elliptical. The lumen becomes narrower from the entrance to the end of the cartilaginous portion, but widens again in the bony portion. The lower wall forms with the tympanic membrane an acute angled depression.
The lumen of the meatus is lined by a prolongation of the external skin of the auricle, this also, greatly diminished in thickness, covering the outer surface of the tympanic membrane, forming its cutaneous layer. In the region of the bony portion the invaginated integument is thin and firmly united with the periosteum, but in the cartilaginous portion it is thicker and, in addition to fine hairs and the sebaceous glands associated with these, has ceruminous glands, secreting a waxy substance.
(Fig. C332, C333, C334, C335, C336, C337, C338)
The foundation of the auricle is a frame-work of elastic cartilage, the majority of whose parts may be made out from the exterior. The sharp curved border that forms the posterior, upper and upper part of the anterior circumference of the auricle is termed the helix. The almost transverse terminal part of the anterior part of the helix is termed its crus, and an anteriorly projecting nodule is termed the spina helicis. Posteriorly and below, the helix passes into a free, flattened cauda helicis. Parallel to the helix is the anthelix, which begins above by two crura, below the highest point of the helix, the depression between the crura being termed the fossa triangularis. The elongated deep groove between the helix and anthelix is the scapha.
The deep depression between the anthelix, the anterior portion of the helix, and the tragus, the actual bottom of the auricular cartilage, is termed the concha. From it the crus of the helix takes its origin and divides the concha into the cymba, between the crus of the helix and the anthelix, and the actual vestibule of the external auditory meatus, the cavum conchae, which is bounded anteriorly by the tragus. The lower, anterior portion of the cartilage is formed by the lamina tragi and the cartilage of the external meatus. The former, together with the integument covering it, forms the tragus and is continued medially into the cartilage of the meatus without any sharp boundary. Opposite the lamina tragi the auricular cartilage is folded so as to produce an elevation, the anti-tragus, which is separated from the cauda helicis by the fissura antitrago-helicina and from the lamina tragi by the incisura intertragica. This incisure produces the narrow isthmus that joins the cartilage of the external meatus and the lamina tragi on the one side with the main: portion of the auricular cartilage on the other, these two portions of the cartilage being separated medially by the incisura terminalis. The depressions of the lateral surface of the auricular cartilage produce corresponding elevations on the medial surface, the eminences of the fossa triangularis, concha and scapha. The first two are separated by the transverse sulcus of the anthelix, a groove that corresponds to the lower crus of the anthelix and passes into the fossa anthelicis, which corresponds to the anthelix. Further, the medial surface has a sulcus of the crus helicis, corresponding to the projection of that name on the lateral surface.
The cartilage of the external auditory meatus begins at its lateral end in the lamina tragi and is a trough-like semicanal whose posterior and upper portion is bridged over by connective tissue. Its continuity is interrupted by, usually, two vertical incisures, the incisures of Santorini, which, also, are bridged over by connective tissue.
The external skin of the ear covers the auricular cartilage so that almost all the irregularities of its surface are clearly to be made out. This depends on the fact that the skin of the auricle is destitute of fat and is consequently closely moulded to the surface of the cartilage. Departures from these conditions are found only at the following places; firstly in the lobe of the ear; this contains no cartilage, but is a duplicature of the integument filled with fat tissue; secondly, the antitrago-helicine fissure and the portion of the terminal incisure between the crus of the helix and the lamina of the tragus are bridged over by the external skin. Over the antitrago-helicine fissure there is a shallow groove, the posterior auricular sulcus, and at the terminal incisure there is a simple groove, the anterior incisure, along which the skin of the auricle passes into that of the cheek. While the lateral surface of the auricle is completely covered with skin, this is the case with only the upper and posterior parts of the medial surface, the skin being reflected from these into the skin of the temporal region (Fig. C336).
In addition to the three parts of the Auricular muscle (see here) that serve for the movement of the auricle, there are some very small muscles on the auricle itself (Fig. C337, C338). The m. helicis major is an elongated flat muscle, which extends from the spine of the helix to where the anterior portion of the helix passes into its upper portion. The m. helicis minor lies on the crus of the helix; it is shorter than the preceding and runs upwards and forwards. The m. tragicus is broadly rectangular; it arises from the lamina of the tragus and runs thence upwards. The m. antitragicus lies on the antitragus behind the incisura anthelicis and unites the antitragus and anthelix. The m. transversus auriculae consists of short fibres, often separated by intervals into distinct bundles, that lie on the medial surface of the auricular cartilage where it unites the eminence of the concha and scapha. The m. obliquus auriculae is a small, weak bundle that unites the eminence of the triangular fossa and that of the concha.
A distinction may be made between the skin itself and the structures formed from it.
The skin consists of three layers, which, named from without inwards, are the cellular layer, the epidermis, the fibrous layer, the corium (dermis or cutis), and the fatty or fascial layer, the tela subcutanea.
The epidermis is the epithelial portion of the skin and is the layer from which all the accessory glandular structures are formed. It varies greatly in thickness in the different regions of the body, its greatest thickness being found on the palm of the hand and the sole of the foot, while it is very thin over the eyelids, the prepuce, the scrotum, etc. Just as the corium passes into the mucous membrane at the body openings, so too the epidermis passes into the epithelium of the membranes.
The corium (dermis or cutis) has numerous furrows, the sulci cutis, upon its outer surface, these being sometimes faint, sometimes deeper. In many regions of the body, such as the palmar surface of the hand or the sole of the foot, where they are especially well developed and regularly arranged, the sulci are separated by distinct ridges, the cristae cutis, which form characteristic patterns whose form and arrangement differ in each individual (Fig. C344). Also the thickness of the cutis which is formed by the felt-like interweaving of bundles of connective tissue fibres, varies in different parts of the body, usually in correspondence with the thickness of the epidermis. Numerous elastic fibres in the corium give the skin a high degree of elasticity. Smooth muscle fibres also occur in the skin, forming in some places, such as the tunica dartos of the scrotum and the nipple area of the breast (see here), continuous sheets.
The tela subcutanea passes gradually into the corium, from which strong bundles of connective tissue fibres, the retinacula cutis, project into it. It is separated from the underlying tissues by a thin membrane, the superficial fascia. In most of the regions of the body the tela subcutanea contains more or less fat, this constituting what is termed the panniculus adiposus. Only at definite individual regions is the skin destitute of fat tissue (the eyelids, the scrotum, the prepuce, labia minora, the auricle, etc.).
The mammary glands (Fig. C340, C341, C342, C343), which are developments of the integument, are peculiarly modified sudoriferous glands, which, in the completely developed and functioning condition, secrete milk. They are paired and lie in the fat tissue of the skin of the anterior thoracic wall. The glandular tissue proper and the subcutaneous fat form together the breast, mamma, varying greatly in its prominence in different individuals. The glandular substance of each gland has a flattened, hemispherical form, and consists of 15-24 irregularly shaped lobes, more or less deeply separated by fat tissue. Each lobe again is composed of small lobules and has a special excretory duct, the ductus lactiferus, which opens upon the nipple.
The nipple (papilla mammae) (Fig. C340) lies in the center of a circular darkly pigmented area of skin, the areola mammae, which is characterized by the absence of fat and by the presence over its surface of large sebaceous glands, the areolar (Montgomery's) glands, each of which forms a small wart-like elevation. The nipple is conical and varies greatly in height and size in different individuals; it is covered by a delicate, much wrinkled skin and is especially rich in smooth muscle fibres. On its summit the lactiferous ducts (Fig. C343) from the lobes of the gland open by small pores; each duct, shortly before its opening, undergoing a spindle-shaped enlargement, the sinus lactiferus.
The mammary glands are situated at the level of the third to the sixth or seventh rib, in the mammary region. The level of the nipple varies greatly; usually it corresponds to the fourth intercostal space. The glandular substance has no sharp delimitation at its periphery and, frequently, prolongations of it extend towards the axillary cavity. It is separated from the Pectoralis major by the fascia of that muscle.
In the male the actual mammary gland is rudimentary; only the nipple is developed.
The nails (Fig. C346, C347, C348, C349, C350) are thin, translucent, horny plates, situated on the dorsal surface of the terminal phalanges of the fingers and toes. Their number is, accordingly, 20. Each is strongly curved in the direction transverse to the axis of the phalanx, so that the dorsal surface is convex. The greater part of this surface of the nail is uncovered, and the nail projects as a free border over the distal extremity of the phalanx. The proximal thinner portion, the root (radix), lies in a fold of skin and ends in a sharp, usually convex margo occultus, while the lateral borders are also imbedded in folds of skin. At the transition of the root into the body of the nail there is a whitish, semilunar area, the lunula, which is the portion of the formative area of the nail that projects beyond the nail wall. The upper convex surface of the nail is smooth, but the under surface is finely striated longitudinally, and on this surface the horny nail substance passes without delimitation into the uncornified germinal layer of the epidermis.
The surface of the phalanx upon which the concave under surface of the nail rests is termed the nail bed (matrix unguis), and is a portion of the skin destitute of glands and fastened by strong bundles of connective tissue to the ungicular tuberosity of the terminal phalanx. On the surface turned toward the nail it shows longitudinal ridges (cristae matricis). The groove of the skin in which the root and posterior part of the lateral borders of the nail are lodged is termed the sulcus of the matrix, and the fold of skin which partly covers these parts is termed the nail wall (vallum unguis). Throughout the greatest part of its length the nail is firmly adherent to the nail bed, only its distal portion being free on both surfaces.
The hairs (Fig. C351, C353) are fine, but long, thread-like, cornified structures of the integument, of which a portion, the scapus, projects freely from the surface of the skin, while the root (radix) is imbedded in the skin, enclosed by a hair follicle. At the bottom of the follicle the hair is attached to a papilla.
Two varieties of hair are found on the skin, the lanugo (Fig. C353) and the stronger body hairs. The lanugo hairs are either very fine or if somewhat coarser they are always quite short; they occur on almost all regions of the skin, but are never closely set. Absolutely destitute of hairs are only the skin of the volar surface of the hand, the plantar surface of the foot, the corresponding surfaces of the fingers and toes and, in addition, the dorsal surface of the terminal phalanges of the fingers and toes, the glans penis, the inner surface of the prepuce and the labia majora, the labia minora and the red portion of the lips.
The stronger body hairs are distinguished by their greater thickness, especially by being more closely set and, usually, by their greater length. They include the eyebrows, supercilia; the eyelashes, cilia; the hairs of the nostrils, vibrissae; the hairs of the auricle, tragi; somewhat longer are the hairs of the scalp, capilli; the beard, barba; the hairs of the pubic region, pubes; and the hairs of the axilla, hirci. The stronger body hairs usually are arranged in groups, as is the case with the hairs of the head. On the bodies of embryos the hairs are arranged in distinct curved lines, termed hair streams (flumina pilorum), which occasionally, as at the crown of the head, become vortices.
Sudoriferous glands (Fig. C352) occur in almost all regions of the skin. Those of the axilla are especially large, as are also the ciliary glands (Glands of Moll) of the eyelids, the circumanal glands and the ceruminous glands of the external auditory meatus.
Sebaceous glands occur in connection with the hair follicles; they are imbedded in the corium and secrete an oily substance, the cutaneous sebum, into the follicles. They are absent from those regions where hairs are lacking, such as the palm of the hand and the sole of the foot.
All the lymph vessels of the pelvis and of the lower extremity drain on either side into the lumbar trunk, which takes origin from the lumbar plexus. This is formed by the union of vessels from the hypogastric plexus of the pelvis with vessels from the lower extremity, which form the external iliac plexus.
If you would like to buy an e-book version of the atlas, available for offline reading and without ads, you can do so in the Amazon Kindle and Google Play stores.


Share